Emre Kudu, Mustafa Altun, Faruk Danış, Sinan Karacabey, Erkman Sanri, Arzu Denizbasi
{"title":"Validating the falls decision rule: optimizing head CT use in older adults with ground-level falls.","authors":"Emre Kudu, Mustafa Altun, Faruk Danış, Sinan Karacabey, Erkman Sanri, Arzu Denizbasi","doi":"10.1007/s43678-025-00937-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Falls are a leading cause of traumatic brain injury in older adults, with ground-level falls being the most common mechanism. Despite the increasing use of head computed tomography (CT) in older adults with ground-level falls, there is an ongoing debate regarding the necessity of routine neuroimaging in all cases. The falls decision rule was developed to safely exclude clinically important intracranial bleeding without head CT in older adults. This study aims to validate the falls decision rule externally and assess its accuracy in identifying low-risk patients while reducing unnecessary imaging.</p><p><strong>Methods: </strong>This prospective cohort study at a Level-1 trauma center enrolled consecutive patients aged ≥ 65 years presenting within 48 h of a ground-level fall. Patient management, including the decision to perform head CT, was determined independently by the treating emergency physician. Patients were followed up for 42 days to identify clinically important intracranial bleeding cases. The rule's diagnostic performance was evaluated using sensitivity, specificity, and predictive values using 95% confidence intervals (CI).</p><p><strong>Results: </strong>A total of 800 patients were included, with a median age of 78 years (IQR 72-85), and 59.9% were female. Clinically important intracranial bleeding was identified in 6.1% (n = 49) of patients. Head CT was performed in 67.6% of cases, identifying 43 initial hemorrhages, with six additional cases detected during follow-ups. The falls decision rule demonstrated 97.9% sensitivity (95% CI 89.1-99.9), 31.9% specificity (95% CI 28.6-35.4), and 99.5% negative predictive value (95% CI 97.1-99.9), potentially reducing CTs by one-third.</p><p><strong>Conclusion: </strong>This validation confirms the falls decision rule's high sensitivity and negative predictive value for identifying low-risk older adults after ground-level falls, potentially reducing unnecessary CT scans by approximately one-third. This approach could alleviate ED overcrowding and resource strain while ensuring diagnostic safety.</p>","PeriodicalId":93937,"journal":{"name":"CJEM","volume":" ","pages":"629-637"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12380872/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CJEM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s43678-025-00937-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/13 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Falls are a leading cause of traumatic brain injury in older adults, with ground-level falls being the most common mechanism. Despite the increasing use of head computed tomography (CT) in older adults with ground-level falls, there is an ongoing debate regarding the necessity of routine neuroimaging in all cases. The falls decision rule was developed to safely exclude clinically important intracranial bleeding without head CT in older adults. This study aims to validate the falls decision rule externally and assess its accuracy in identifying low-risk patients while reducing unnecessary imaging.
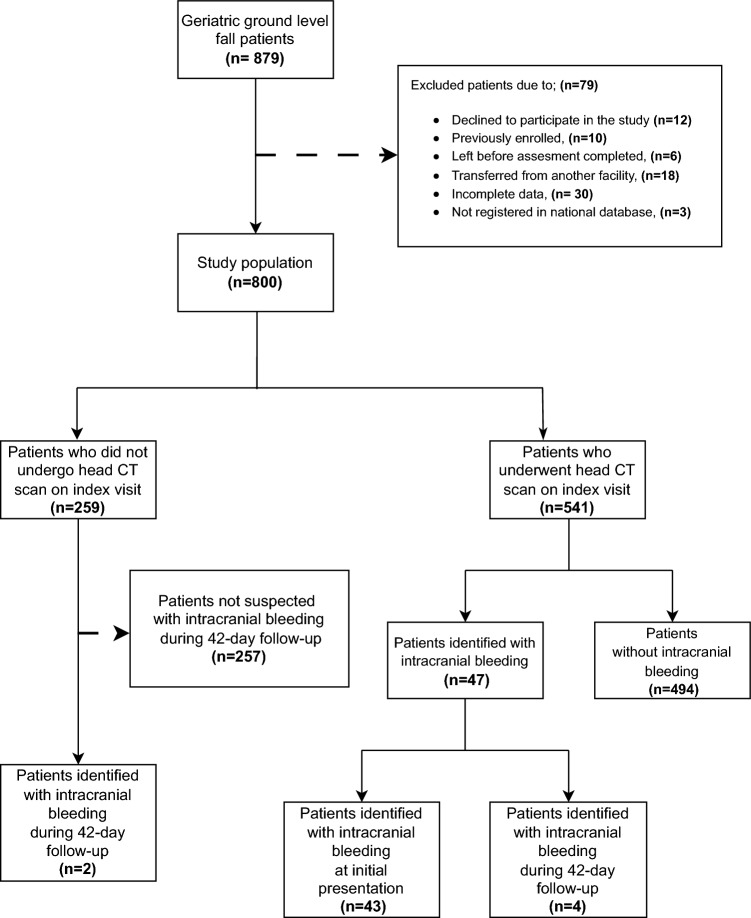
Methods: This prospective cohort study at a Level-1 trauma center enrolled consecutive patients aged ≥ 65 years presenting within 48 h of a ground-level fall. Patient management, including the decision to perform head CT, was determined independently by the treating emergency physician. Patients were followed up for 42 days to identify clinically important intracranial bleeding cases. The rule's diagnostic performance was evaluated using sensitivity, specificity, and predictive values using 95% confidence intervals (CI).
Results: A total of 800 patients were included, with a median age of 78 years (IQR 72-85), and 59.9% were female. Clinically important intracranial bleeding was identified in 6.1% (n = 49) of patients. Head CT was performed in 67.6% of cases, identifying 43 initial hemorrhages, with six additional cases detected during follow-ups. The falls decision rule demonstrated 97.9% sensitivity (95% CI 89.1-99.9), 31.9% specificity (95% CI 28.6-35.4), and 99.5% negative predictive value (95% CI 97.1-99.9), potentially reducing CTs by one-third.
Conclusion: This validation confirms the falls decision rule's high sensitivity and negative predictive value for identifying low-risk older adults after ground-level falls, potentially reducing unnecessary CT scans by approximately one-third. This approach could alleviate ED overcrowding and resource strain while ensuring diagnostic safety.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


