{"title":"Cost-effectiveness of newborn screening for severe combined immunodeficiency: a systematic review.","authors":"Rezwanul Rana, Syed Afroz Keramat, Moin Ahmed","doi":"10.3345/cep.2025.00052","DOIUrl":null,"url":null,"abstract":"<p><p>Severe combined immunodeficiency (SCID) is a rare genetic disorder that causes severe infections and death in early childhood. Newborn bloodspot screening (NBS) for SCID using the T-cell receptor excision circle assay can revolutionize the early detection and treatment of infants with SCID, leading to improved quality of life and life expectancy. This systematic review aimed to examine the cost-effectiveness of universal NBS for SCID. The MEDLINE, Embase, National Health Service (NHS) Economic Evaluation Database, Health Technology Assessment, Scopus, and EconLit databases were searched for studies of the NBS for SCID published between January 2008 and March 2024. A standardized data extraction form was used to gather pertinent data such as characteristics, design, perspective, screening strategies and costs, health outcomes, incremental cost-effectiveness ratios, and sources of uncertainty. Eight studies met our inclusion criteria: 6 cost-utility analyses and 2 cost-effectiveness analyses. All studies were model-based economic evaluations. These studies indicated that universal NBS for SCID is highly likely to demonstrate health system and societal cost-effectiveness. The incremental cost-effectiveness ratio per quality-adjusted life-year gained ranged from $30,214 to $54,282 (United States dollars 2022 value). Evidence suggests that early treatment of SCID is beneficial and that population-based NBS provides good value for the money. However, policymakers require better information about optimal treatment and treatment and screening costs to make informed decisions regarding competing healthcare priorities.</p>","PeriodicalId":36018,"journal":{"name":"Clinical and Experimental Pediatrics","volume":" ","pages":"628-640"},"PeriodicalIF":3.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12409193/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3345/cep.2025.00052","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
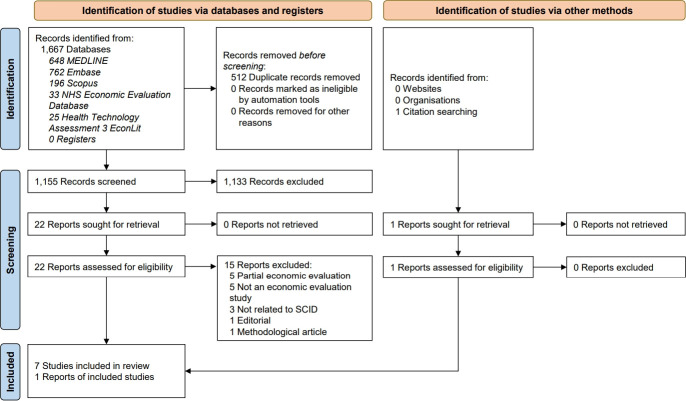
Severe combined immunodeficiency (SCID) is a rare genetic disorder that causes severe infections and death in early childhood. Newborn bloodspot screening (NBS) for SCID using the T-cell receptor excision circle assay can revolutionize the early detection and treatment of infants with SCID, leading to improved quality of life and life expectancy. This systematic review aimed to examine the cost-effectiveness of universal NBS for SCID. The MEDLINE, Embase, National Health Service (NHS) Economic Evaluation Database, Health Technology Assessment, Scopus, and EconLit databases were searched for studies of the NBS for SCID published between January 2008 and March 2024. A standardized data extraction form was used to gather pertinent data such as characteristics, design, perspective, screening strategies and costs, health outcomes, incremental cost-effectiveness ratios, and sources of uncertainty. Eight studies met our inclusion criteria: 6 cost-utility analyses and 2 cost-effectiveness analyses. All studies were model-based economic evaluations. These studies indicated that universal NBS for SCID is highly likely to demonstrate health system and societal cost-effectiveness. The incremental cost-effectiveness ratio per quality-adjusted life-year gained ranged from $30,214 to $54,282 (United States dollars 2022 value). Evidence suggests that early treatment of SCID is beneficial and that population-based NBS provides good value for the money. However, policymakers require better information about optimal treatment and treatment and screening costs to make informed decisions regarding competing healthcare priorities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


