{"title":"The utilization of percutaneous endoscopic lumbar discectomy in recurrent lumbar disc herniation: a systematic review and meta-analysis.","authors":"Saiganesh Ravikumar, Aaron Bloschichak, Sanjeev Kumar","doi":"10.21037/jss-24-47","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The utilization of percutaneous endoscopic lumbar discectomy (PELD) in lumbar disc herniation (LDH) is well established as a safe, effective intervention. However, in approximately 5-15% of cases herniation recurs. The role of PELD at this juncture is not well established in literature. The aim of this study is to identify the usability of PELD in comparison to other minimally invasive options to treat recurrent lumbar herniated disc.</p><p><strong>Methods: </strong>We searched the PubMed, EMBASE, and Web of Science. Studies with less than 10 patients, published abstracts without full texts, and systematic review papers were excluded. Both transforaminal (TF) and interlaminar (IL) approaches were included. A risk of bias assessment was performed for each study.</p><p><strong>Results: </strong>A total of 614 non-duplicate articles resulted. After applying inclusion/exclusion criteria, 20 papers were selected. Eleven studies were cohort, 1 study was randomized controlled trial, 8 studies were case-series. There were a total of 1,162 patients and 1,165 discs operated on. 714 (61.3%) surgeries were at level L4-5, 390 (33.4%) surgeries were at level L5-S1, and 62 (5.32%) surgeries were at other lumbar levels. 15 studies reported average visual analog scale (VAS) scores or Numerical Rating Score (NRS) of back and leg pain. Pooled weighted averages illustrated a 5.24-point improvement in VAS back scores and a similar 5.26-point improvement in VAS leg scores. Oswestry Disability Index (ODI) was reported in 5 studies with a pooled weighted average ODI showing an improvement of 20.88 units. All studies reported complications encountered, and the pooled rate across studies were: dural tear (n=10, 0.88%), infection (n=1, 0.09%), transient dysesthesia (n=13, 1.14%), transient headache (n=5, 0.44%), instability (n=8, 0.70%), persistent leg pain (n=7, 0.62%), transient weakness (n=1, 0.09%) permanent neurologic deficit (n=1, 0.09%). Seventeen studies (85%) reported re-recurrence rates of herniated disc after PELD, with a total of 58 recurrences out of 1,018 discs, or 5.70% pooled recurrence rate. A meta-analysis revealed there is currently no evidence of clearly superior approach for managing recurrent LDH between open lumbar microdiscectomy, minimally invasive trans-lumbar interbody fusion, microendoscopic discectomy, and IL <i>vs</i>. TF approach of PELD.</p><p><strong>Conclusions: </strong>PELD is a safe, effective technique in the treatment of recurrent LDH. Clinical judgment is required at this time to identify the best surgical modality of management for each patient.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"11 1","pages":"45-64"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11998055/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-47","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The utilization of percutaneous endoscopic lumbar discectomy (PELD) in lumbar disc herniation (LDH) is well established as a safe, effective intervention. However, in approximately 5-15% of cases herniation recurs. The role of PELD at this juncture is not well established in literature. The aim of this study is to identify the usability of PELD in comparison to other minimally invasive options to treat recurrent lumbar herniated disc.
Methods: We searched the PubMed, EMBASE, and Web of Science. Studies with less than 10 patients, published abstracts without full texts, and systematic review papers were excluded. Both transforaminal (TF) and interlaminar (IL) approaches were included. A risk of bias assessment was performed for each study.
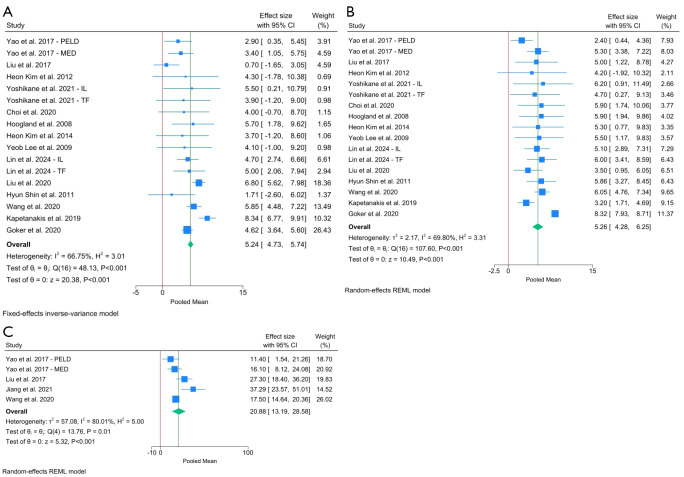
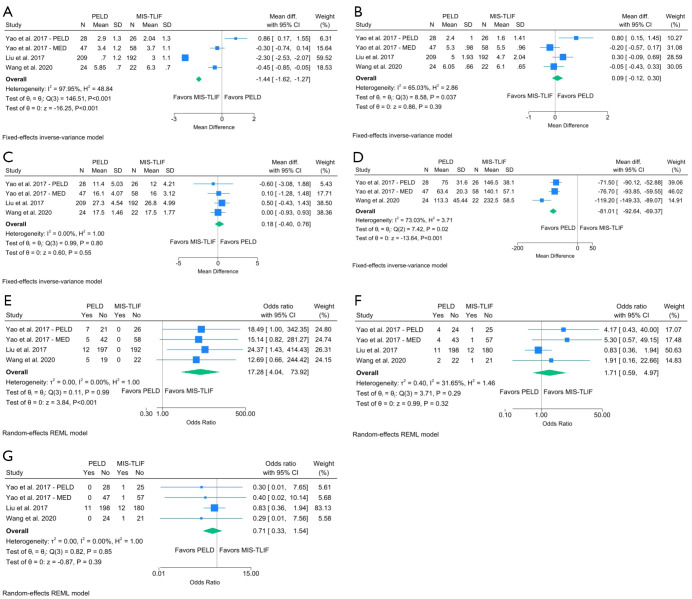
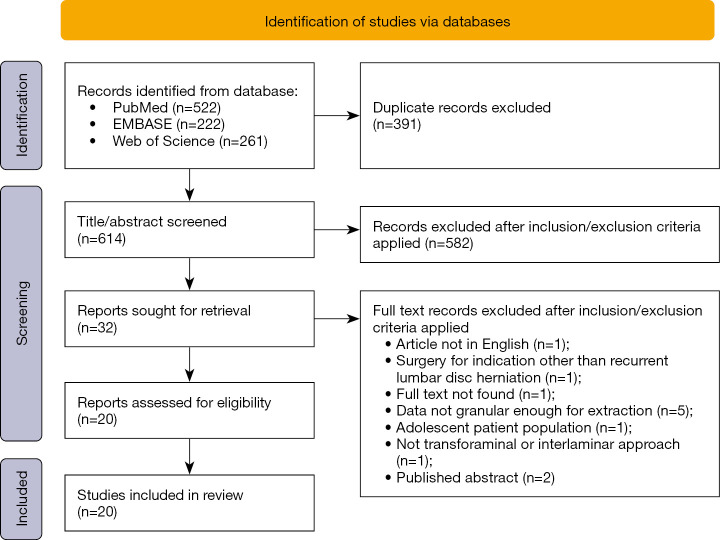
Results: A total of 614 non-duplicate articles resulted. After applying inclusion/exclusion criteria, 20 papers were selected. Eleven studies were cohort, 1 study was randomized controlled trial, 8 studies were case-series. There were a total of 1,162 patients and 1,165 discs operated on. 714 (61.3%) surgeries were at level L4-5, 390 (33.4%) surgeries were at level L5-S1, and 62 (5.32%) surgeries were at other lumbar levels. 15 studies reported average visual analog scale (VAS) scores or Numerical Rating Score (NRS) of back and leg pain. Pooled weighted averages illustrated a 5.24-point improvement in VAS back scores and a similar 5.26-point improvement in VAS leg scores. Oswestry Disability Index (ODI) was reported in 5 studies with a pooled weighted average ODI showing an improvement of 20.88 units. All studies reported complications encountered, and the pooled rate across studies were: dural tear (n=10, 0.88%), infection (n=1, 0.09%), transient dysesthesia (n=13, 1.14%), transient headache (n=5, 0.44%), instability (n=8, 0.70%), persistent leg pain (n=7, 0.62%), transient weakness (n=1, 0.09%) permanent neurologic deficit (n=1, 0.09%). Seventeen studies (85%) reported re-recurrence rates of herniated disc after PELD, with a total of 58 recurrences out of 1,018 discs, or 5.70% pooled recurrence rate. A meta-analysis revealed there is currently no evidence of clearly superior approach for managing recurrent LDH between open lumbar microdiscectomy, minimally invasive trans-lumbar interbody fusion, microendoscopic discectomy, and IL vs. TF approach of PELD.
Conclusions: PELD is a safe, effective technique in the treatment of recurrent LDH. Clinical judgment is required at this time to identify the best surgical modality of management for each patient.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


