Work-in-progress report: a prospective, multi-institutional observational study on intraoperative lymph node dissection for thymic epithelial malignancies with radiologically invasive features.
{"title":"Work-in-progress report: a prospective, multi-institutional observational study on intraoperative lymph node dissection for thymic epithelial malignancies with radiologically invasive features.","authors":"Masatsugu Hamaji, Shigeto Nishikawa, Sho Koyasu, Yojiro Yutaka, Fumitsugu Kojima, Takao Nakanishi, Tomoya Kono, Yoshito Yamada, Kyoko Hijiya, Keiji Ohata, Ryutaro Kikuchi, Ei Miyamoto, Tatsuo Nakagawa, Mitsugu Omasa, Ryo Miyahara, Toru Bando, Hiroshi Date","doi":"10.21037/med-24-42","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although lymph node metastasis may be an adverse prognostic factor for survival after resection of thymic epithelial malignancies, recommendations for intraoperative lymph node dissection (LND) lack consistency across various guidelines. This study aimed to investigate feasibility and characteristics of LND.</p><p><strong>Methods: </strong>This is a work-in-progress report of our prospective, multi-institutional observational study to evaluate the feasibility and characteristics of LND in patients with resectable thymic epithelial malignancies that exhibit radiological invasive features such as size >5 cm, standardized uptake value >5, or suspected invasion of surrounding organs.</p><p><strong>Results: </strong>In total, 25 patients were enrolled in this study. All patients underwent complete resection of the primary lesion with N1-level or N2-level LND. Among these, 22 (88%) patients underwent N1-level LND, and 20 (80%) patients underwent N2-level LND. No significant differences between the open and minimally invasive approaches were observed in the number of dissected stations (P=0.71), N1-level LND (P=0.49), or N2-level LND (P=0.69).</p><p><strong>Conclusions: </strong>Intraoperative LND may be feasible in both approaches and may contribute to accurate nodal staging in resectable thymic malignancies with radiologically invasive features.</p>","PeriodicalId":74139,"journal":{"name":"Mediastinum (Hong Kong, China)","volume":"9 ","pages":"2"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11982983/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediastinum (Hong Kong, China)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/med-24-42","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although lymph node metastasis may be an adverse prognostic factor for survival after resection of thymic epithelial malignancies, recommendations for intraoperative lymph node dissection (LND) lack consistency across various guidelines. This study aimed to investigate feasibility and characteristics of LND.
Methods: This is a work-in-progress report of our prospective, multi-institutional observational study to evaluate the feasibility and characteristics of LND in patients with resectable thymic epithelial malignancies that exhibit radiological invasive features such as size >5 cm, standardized uptake value >5, or suspected invasion of surrounding organs.
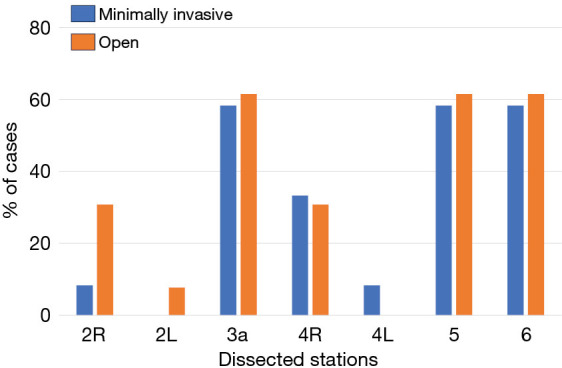
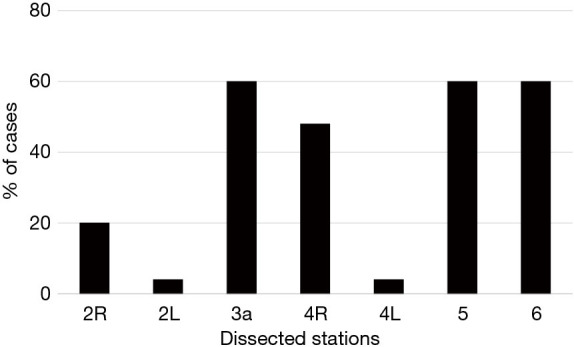
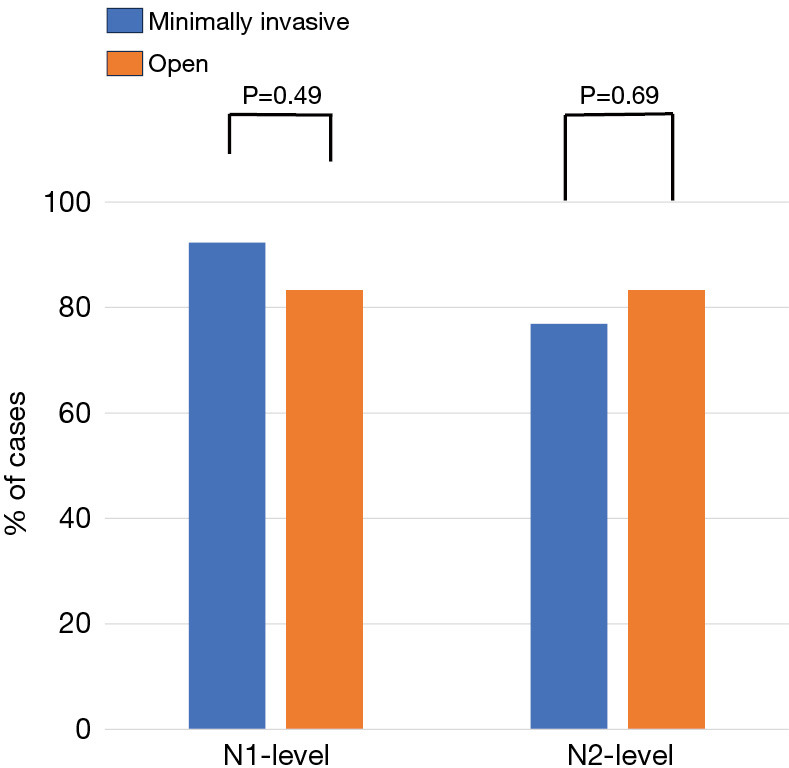
Results: In total, 25 patients were enrolled in this study. All patients underwent complete resection of the primary lesion with N1-level or N2-level LND. Among these, 22 (88%) patients underwent N1-level LND, and 20 (80%) patients underwent N2-level LND. No significant differences between the open and minimally invasive approaches were observed in the number of dissected stations (P=0.71), N1-level LND (P=0.49), or N2-level LND (P=0.69).
Conclusions: Intraoperative LND may be feasible in both approaches and may contribute to accurate nodal staging in resectable thymic malignancies with radiologically invasive features.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


