Eric A Klein, Timothy R Church, Christina A Clarke, Earl Hubbell
{"title":"Modeled Benefit of Individual Cancer Signal Origin Prediction for Multi-Cancer Early Detection.","authors":"Eric A Klein, Timothy R Church, Christina A Clarke, Earl Hubbell","doi":"10.1158/2767-9764.CRC-24-0351","DOIUrl":null,"url":null,"abstract":"<p><p>Multi-cancer early detection (MCED) tests may detect a broad spectrum of cancer types, including uncommon types that lack recommended screening. After a cancer signal is detected by an MCED test, some diagnostic process must definitively confirm the patient's cancer status. A commercially available blood-based MCED test detects a cancer signal and then predicts an anatomic location, a cancer signal origin (CSO), to guide the diagnostic process. We extended a preexisting model for MCED cancer screening, adding predicted CSO categories and a simple model of the diagnostic chain. We then predicted outcomes of the diagnostic chain for each predicted CSO and in populations with differing clinical risk factors. Typical positive predictive values were>40%, and using a minimal sufficient level of positive predictive value (>7%), (i) diagnostic workup based on any CSO was generally warranted, and (ii) continued workup for cancers in locations other than the CSO was justifiable. The benefit of prediction-directed workups was also observed via estimated clinical utility metrics, such as lives saved per diagnostic test, and remained applicable in populations with varying cancer risk, such as lung cancer prediction-directed workups in never-smokers. CSO predictions may enable most true-positive cases to be resolved by short and efficient diagnostic processes. The model predicted a large enough conditional benefit to warrant diagnostic workup based on any CSO prediction from an MCED test, assuming late-stage reduction by MCED leads to mortality reduction, which remains to be demonstrated.</p><p><strong>Significance: </strong>MCED tests may detect a signal from many cancers. Predicting an anatomic location from which the cancer signal may originate allows effective, usual diagnostic workup. In this study, we show that these predictions are beneficial to physicians choosing a diagnostic path, even for uncommon cancer types and among populations with differing cancer risks.</p>","PeriodicalId":72516,"journal":{"name":"Cancer research communications","volume":" ","pages":"814-824"},"PeriodicalIF":3.3000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12087281/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer research communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1158/2767-9764.CRC-24-0351","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
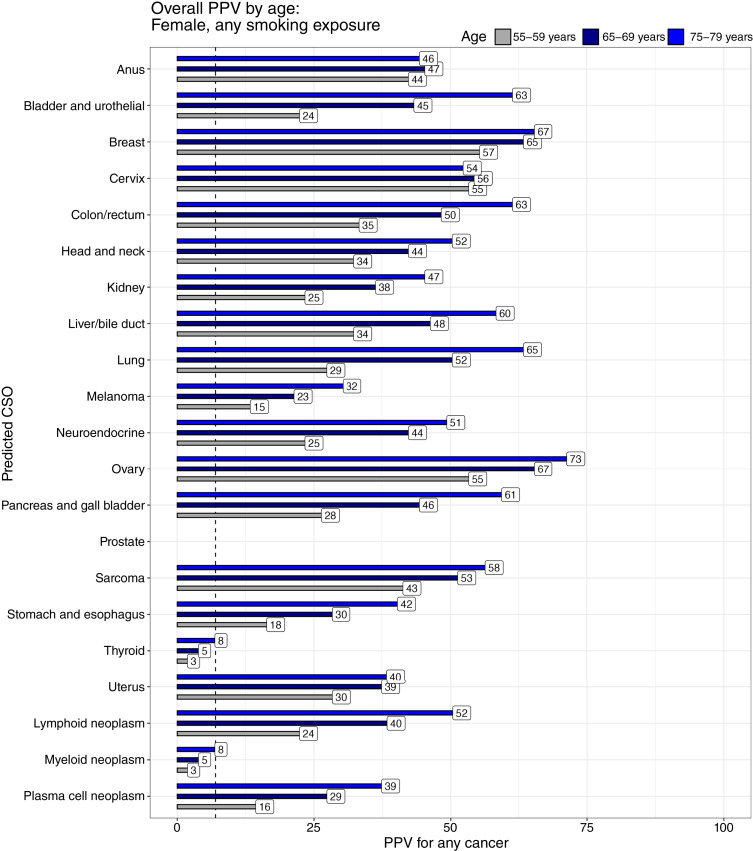
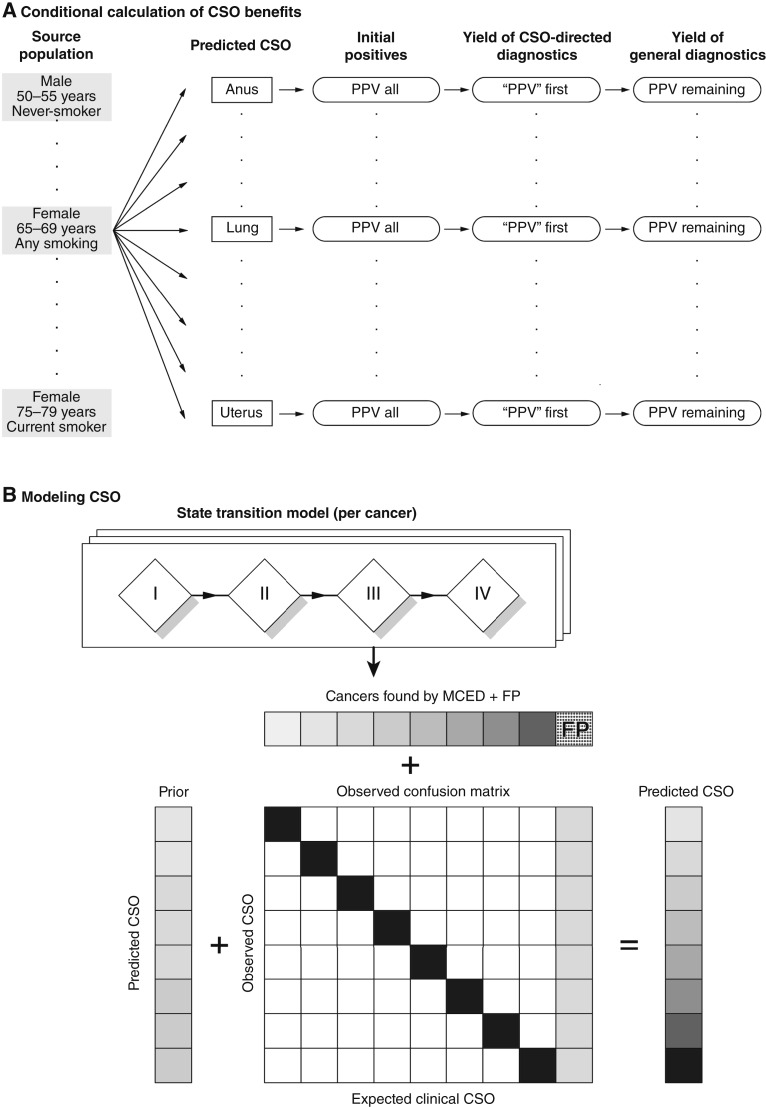
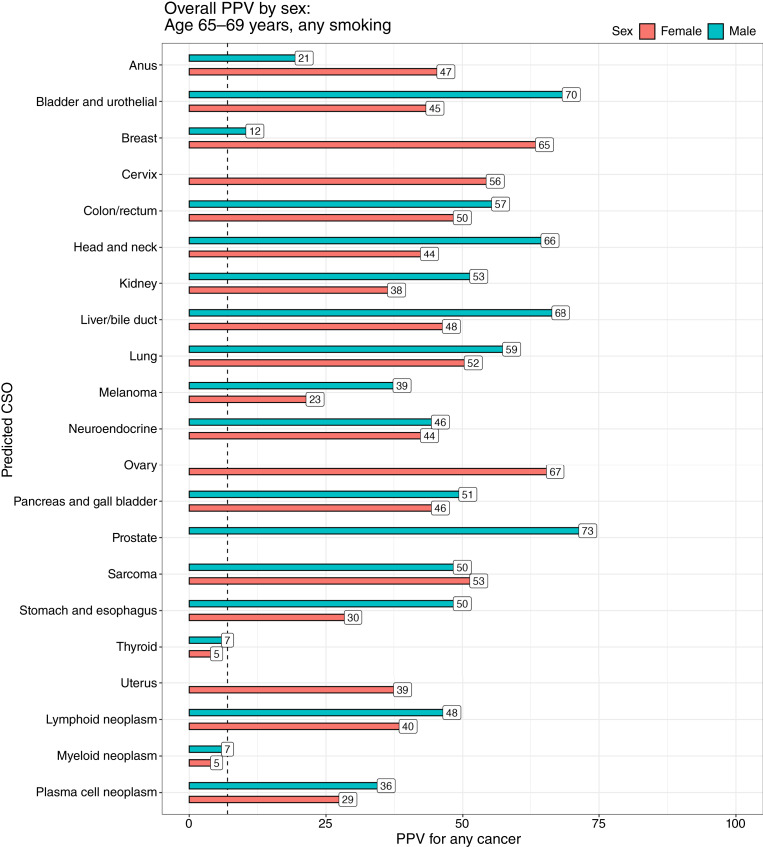
Multi-cancer early detection (MCED) tests may detect a broad spectrum of cancer types, including uncommon types that lack recommended screening. After a cancer signal is detected by an MCED test, some diagnostic process must definitively confirm the patient's cancer status. A commercially available blood-based MCED test detects a cancer signal and then predicts an anatomic location, a cancer signal origin (CSO), to guide the diagnostic process. We extended a preexisting model for MCED cancer screening, adding predicted CSO categories and a simple model of the diagnostic chain. We then predicted outcomes of the diagnostic chain for each predicted CSO and in populations with differing clinical risk factors. Typical positive predictive values were>40%, and using a minimal sufficient level of positive predictive value (>7%), (i) diagnostic workup based on any CSO was generally warranted, and (ii) continued workup for cancers in locations other than the CSO was justifiable. The benefit of prediction-directed workups was also observed via estimated clinical utility metrics, such as lives saved per diagnostic test, and remained applicable in populations with varying cancer risk, such as lung cancer prediction-directed workups in never-smokers. CSO predictions may enable most true-positive cases to be resolved by short and efficient diagnostic processes. The model predicted a large enough conditional benefit to warrant diagnostic workup based on any CSO prediction from an MCED test, assuming late-stage reduction by MCED leads to mortality reduction, which remains to be demonstrated.
Significance: MCED tests may detect a signal from many cancers. Predicting an anatomic location from which the cancer signal may originate allows effective, usual diagnostic workup. In this study, we show that these predictions are beneficial to physicians choosing a diagnostic path, even for uncommon cancer types and among populations with differing cancer risks.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


