Faith Michael, Travis Quevillon, Suzanne Betteridge-LeBlanc, Mustafa Alzahran, Rafael Shehata, Cynthia A Jackevicius, Rony Atoui, Bindu Bittira, Tina Baykaner, Paula Harvey, Ratika Parkash, Jeff S Healey, Dennis T Ko, Mohammed Shurrab
{"title":"Post-cardiac surgery atrial fibrillation and sex differences in clinical outcomes: a systematic review and meta-analysis.","authors":"Faith Michael, Travis Quevillon, Suzanne Betteridge-LeBlanc, Mustafa Alzahran, Rafael Shehata, Cynthia A Jackevicius, Rony Atoui, Bindu Bittira, Tina Baykaner, Paula Harvey, Ratika Parkash, Jeff S Healey, Dennis T Ko, Mohammed Shurrab","doi":"10.1093/ehjopen/oeaf033","DOIUrl":null,"url":null,"abstract":"<p><p>There is conflicting literature on sex differences and clinical outcomes in patients who develop atrial fibrillation (AF) post-cardiac surgery. Our aim was to compare clinical outcomes between females and males with post-cardiac surgery AF. A systematic search was conducted for studies published until 27 September 2024 in MEDLINE, Embase, and CENTRAL. Included studies compared mortality and stroke in females vs. males who developed AF after cardiac surgery. Outcomes of interest were mortality and stroke. Pooled prevalence was used to compare comorbidities. Raw event rates were used to calculate odds ratios (ORs), which were pooled with a fixed-effects model. 10 422 studies were identified and 5 studies met inclusion criteria. 14 970 patients who developed AF after cardiac surgery were included, of whom 3748 were females. The length of follow-up was up to 10 years. The weighted average age was 70.4 ± 2.9 years in females and 66.7 ± 2.4 years in males (<i>P</i> = 0.32). At baseline, females had a higher prevalence of hypertension, diabetes, dyslipidemia, stroke, and peripheral vascular disease. The odds of in-hospital mortality among females were higher compared to males (5.5 vs. 3.0%; OR 2.04, 95% CI 1.42-2.91, <i>P</i> < 0.001, <i>I</i> <sup>2</sup> = 57%). There were no significant differences in post-discharge mortality (45.6 vs. 42.9%; OR 1.05, 95% CI 0.97-1.15, <i>P</i> = 0.23, <i>I</i> <sup>2</sup> = 0%) or in-hospital stroke (2.5 vs. 1.9%; OR 1.30, 95% CI 0.79-2.13, <i>P</i> = 0.30, <i>I</i> <sup>2</sup> = 57%) in females vs. males. In conclusion, females with post-cardiac surgery AF had a higher prevalence of comorbidities at baseline. The odds of in-hospital mortality were twice as high among females. There were no significant differences in post-discharge mortality or in-hospital stroke. Future studies are warranted to understand the mechanisms of increased in-hospital mortality in females and to develop effective monitoring strategies and interventions.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 2","pages":"oeaf033"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11981890/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
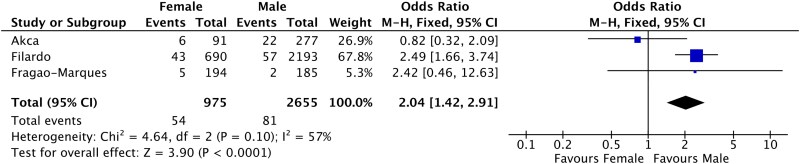
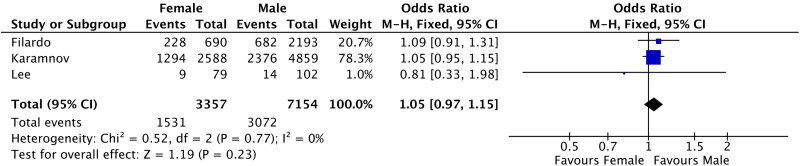
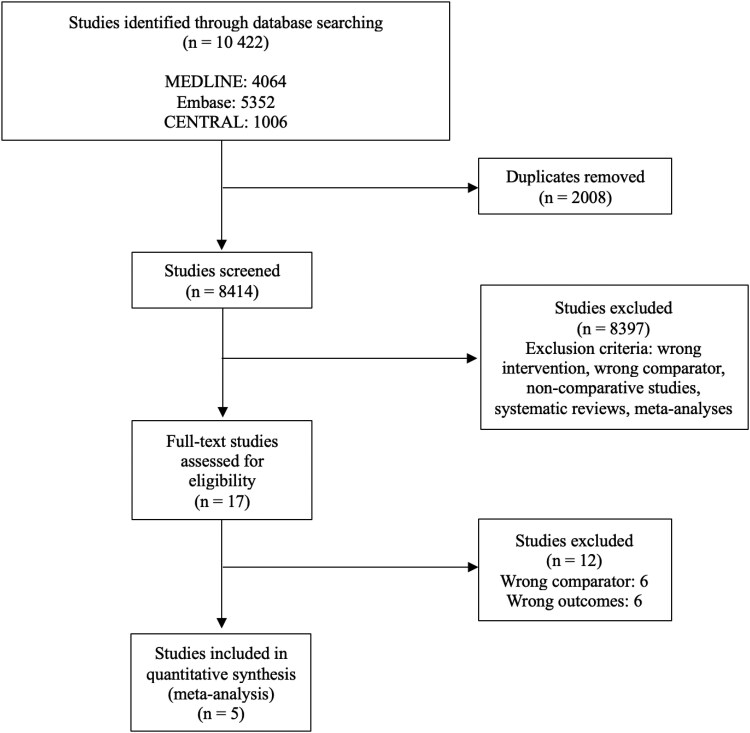
There is conflicting literature on sex differences and clinical outcomes in patients who develop atrial fibrillation (AF) post-cardiac surgery. Our aim was to compare clinical outcomes between females and males with post-cardiac surgery AF. A systematic search was conducted for studies published until 27 September 2024 in MEDLINE, Embase, and CENTRAL. Included studies compared mortality and stroke in females vs. males who developed AF after cardiac surgery. Outcomes of interest were mortality and stroke. Pooled prevalence was used to compare comorbidities. Raw event rates were used to calculate odds ratios (ORs), which were pooled with a fixed-effects model. 10 422 studies were identified and 5 studies met inclusion criteria. 14 970 patients who developed AF after cardiac surgery were included, of whom 3748 were females. The length of follow-up was up to 10 years. The weighted average age was 70.4 ± 2.9 years in females and 66.7 ± 2.4 years in males (P = 0.32). At baseline, females had a higher prevalence of hypertension, diabetes, dyslipidemia, stroke, and peripheral vascular disease. The odds of in-hospital mortality among females were higher compared to males (5.5 vs. 3.0%; OR 2.04, 95% CI 1.42-2.91, P < 0.001, I2 = 57%). There were no significant differences in post-discharge mortality (45.6 vs. 42.9%; OR 1.05, 95% CI 0.97-1.15, P = 0.23, I2 = 0%) or in-hospital stroke (2.5 vs. 1.9%; OR 1.30, 95% CI 0.79-2.13, P = 0.30, I2 = 57%) in females vs. males. In conclusion, females with post-cardiac surgery AF had a higher prevalence of comorbidities at baseline. The odds of in-hospital mortality were twice as high among females. There were no significant differences in post-discharge mortality or in-hospital stroke. Future studies are warranted to understand the mechanisms of increased in-hospital mortality in females and to develop effective monitoring strategies and interventions.
关于心脏手术后发生心房颤动(AF)患者的性别差异和临床结果的文献存在矛盾。我们的目的是比较女性和男性心脏手术后房颤的临床结果。我们对2024年9月27日前在MEDLINE、Embase和CENTRAL上发表的研究进行了系统检索。纳入的研究比较了心脏手术后发生房颤的女性和男性的死亡率和卒中。研究的结果是死亡率和中风。合并患病率用于比较合并症。原始事件率用于计算优势比(ORs),并将其与固定效应模型合并。共纳入10422项研究,其中5项研究符合纳入标准。纳入14970例心脏手术后发生房颤的患者,其中3748例为女性。随访时间长达10年。加权平均年龄女性为70.4±2.9岁,男性为66.7±2.4岁(P = 0.32)。在基线时,女性高血压、糖尿病、血脂异常、中风和周围血管疾病的患病率较高。女性住院死亡率高于男性(5.5%比3.0%;或2.04,95% ci 1.42-2.91, p < 0.001, I 2 = 57%)。两组出院后死亡率无显著差异(45.6% vs 42.9%;OR 1.05, 95% CI 0.97-1.15, P = 0.23, i2 = 0%)或院内卒中(2.5 vs. 1.9%;OR 1.30, 95% CI 0.79-2.13, P = 0.30, i2 = 57%)。综上所述,女性心脏手术后房颤在基线时具有较高的合并症患病率。女性的住院死亡率是男性的两倍。两组在出院后死亡率和院内卒中方面无显著差异。未来的研究有必要了解女性住院死亡率增加的机制,并制定有效的监测策略和干预措施。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


