{"title":"Improved Prediction of Fluid Responsiveness in Ventilated Patients With Low Tidal Volume: The Role of Preload Variation.","authors":"Antonio Gordillo Brenes, Lourdes León Montañés, Benjamín Hernández Alonso, Samer Alarabe Peinado, Ángel Sánchez Rodríguez","doi":"10.1097/CCE.0000000000001259","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To analyze whether two levels of preload, one reduced by the application of tourniquets with sphygmomanometer cuffs and the other increased by passive leg elevation, improve the predictive capacity of pulse pressure variation (PPV) and stroke volume variation (SVV) of fluid responsiveness in patients ventilated with low tidal volume (Vt).</p><p><strong>Design: </strong>Prospective cohort study.</p><p><strong>Setting: </strong>ICU at the University Hospital of Cádiz (Spain).</p><p><strong>Patients: </strong>Patients diagnosed with septic shock, on controlled invasive mechanical ventilation without spontaneous breathing, with a Vt of 6 mL/kg predicted body weight and considered for an intravascular volume load due to hemodynamic instability.</p><p><strong>Interventions: </strong>Patient position changes: supine position and passive leg raise. Placement of pressure cuff compression at 60 mm Hg in one upper limb and the two lower limbs. Administration of 10 mL/kg of saline solution in 10 minutes.</p><p><strong>Measurements and results: </strong>Twenty-eight tests were obtained. The baseline characteristics of the responders and nonresponders were similar. The baseline variables PPV and SVV had a limited ability to predict the response to fluids, with areas under the curve of 0.71 and 0.66, respectively. However, its predictive capacity increases significantly with different maneuvers, with the best prediction of the difference between the PPV value during the application of tourniquets and the PPV value in the supine position, with an area under the receiver operating characteristic curve of 0.97.</p><p><strong>Conclusions: </strong>Lowering preload using tourniquets improves the predictive capacity of PPV and SVV for fluid responsiveness in patients ventilated with low Vt.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 5","pages":"e1259"},"PeriodicalIF":2.7000,"publicationDate":"2025-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12040047/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001259","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To analyze whether two levels of preload, one reduced by the application of tourniquets with sphygmomanometer cuffs and the other increased by passive leg elevation, improve the predictive capacity of pulse pressure variation (PPV) and stroke volume variation (SVV) of fluid responsiveness in patients ventilated with low tidal volume (Vt).
Design: Prospective cohort study.
Setting: ICU at the University Hospital of Cádiz (Spain).
Patients: Patients diagnosed with septic shock, on controlled invasive mechanical ventilation without spontaneous breathing, with a Vt of 6 mL/kg predicted body weight and considered for an intravascular volume load due to hemodynamic instability.
Interventions: Patient position changes: supine position and passive leg raise. Placement of pressure cuff compression at 60 mm Hg in one upper limb and the two lower limbs. Administration of 10 mL/kg of saline solution in 10 minutes.
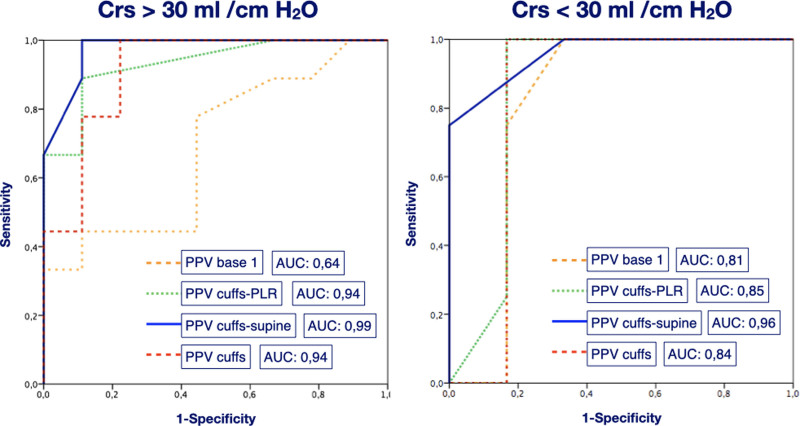
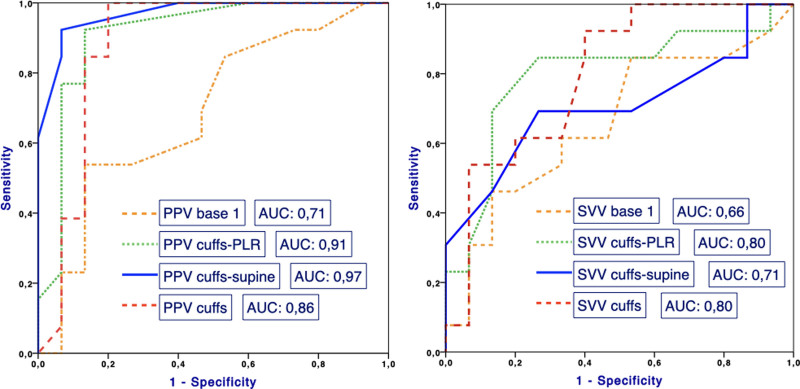
Measurements and results: Twenty-eight tests were obtained. The baseline characteristics of the responders and nonresponders were similar. The baseline variables PPV and SVV had a limited ability to predict the response to fluids, with areas under the curve of 0.71 and 0.66, respectively. However, its predictive capacity increases significantly with different maneuvers, with the best prediction of the difference between the PPV value during the application of tourniquets and the PPV value in the supine position, with an area under the receiver operating characteristic curve of 0.97.
Conclusions: Lowering preload using tourniquets improves the predictive capacity of PPV and SVV for fluid responsiveness in patients ventilated with low Vt.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


