{"title":"The Lost Gallstone: Thoracoscopic Removal of Retained Gallstone Following Cholecystectomy.","authors":"Aulon Jerliu, Brian Wong Won, Alicia McKelvey","doi":"10.4293/CRSLS.2024.00030","DOIUrl":null,"url":null,"abstract":"<p><p>Cholecystectomy, the surgical removal of the gallbladder, is a common abdominal operation often performed laparoscopically due to its minimally invasive nature. Despite its safety and efficacy, rare complications such as gallstone retention outside the biliary system can occur. One unusual complication is the migration of gallstones into the thoracic cavity, potentially causing severe outcomes like pleural effusion, empyema, or bronchopleural fistula, which present diagnostic challenges due to their rarity and varied symptoms. Advanced imaging techniques are essential for diagnosis, while treatment ranges from conservative management for asymptomatic cases to surgical intervention for significant complications. This report details the case of an 80-year-old male who presented with epistaxis and hemoptysis, later found to have a retained thoracic gallstone postcholecystectomy. Despite initial normal imaging and clinical improvement, further investigation revealed a gallstone eroding through the diaphragm into the thoracic cavity. The patient underwent successful thoracoscopic removal of the stone but experienced a prolonged hospital stay due to complications, including atrial fibrillation exacerbation, hemothorax, and lower extremity ischemia. The report underscores the diagnostic complexities of intrathoracic gallstone migration and the severe complications that can arise. A high index of suspicion is necessary for patients with persistent respiratory symptoms following cholecystectomy, and timely imaging and surgical intervention are crucial to minimize morbidity.</p>","PeriodicalId":72723,"journal":{"name":"CRSLS : MIS case reports from SLS","volume":"12 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12038875/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CRSLS : MIS case reports from SLS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4293/CRSLS.2024.00030","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
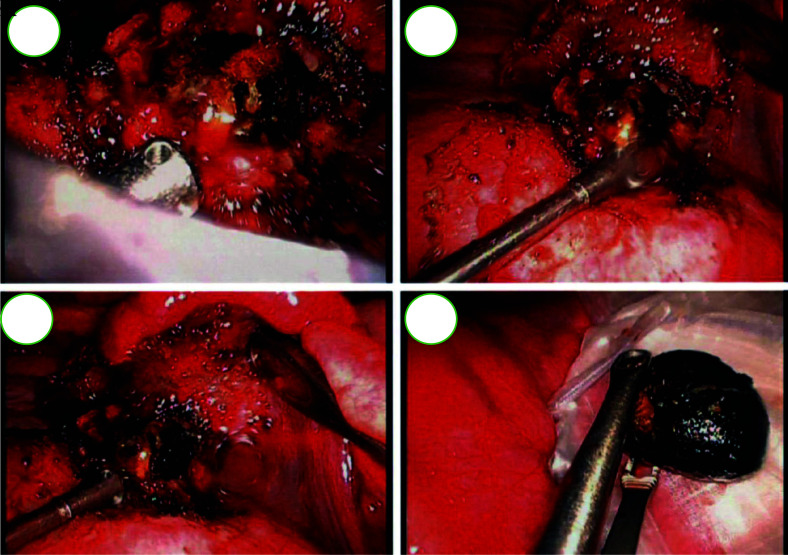
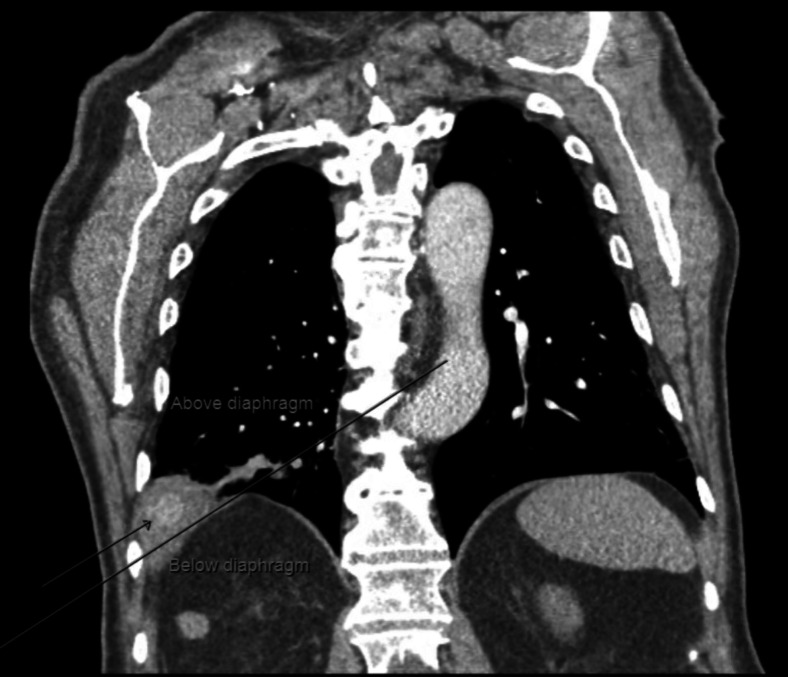
Cholecystectomy, the surgical removal of the gallbladder, is a common abdominal operation often performed laparoscopically due to its minimally invasive nature. Despite its safety and efficacy, rare complications such as gallstone retention outside the biliary system can occur. One unusual complication is the migration of gallstones into the thoracic cavity, potentially causing severe outcomes like pleural effusion, empyema, or bronchopleural fistula, which present diagnostic challenges due to their rarity and varied symptoms. Advanced imaging techniques are essential for diagnosis, while treatment ranges from conservative management for asymptomatic cases to surgical intervention for significant complications. This report details the case of an 80-year-old male who presented with epistaxis and hemoptysis, later found to have a retained thoracic gallstone postcholecystectomy. Despite initial normal imaging and clinical improvement, further investigation revealed a gallstone eroding through the diaphragm into the thoracic cavity. The patient underwent successful thoracoscopic removal of the stone but experienced a prolonged hospital stay due to complications, including atrial fibrillation exacerbation, hemothorax, and lower extremity ischemia. The report underscores the diagnostic complexities of intrathoracic gallstone migration and the severe complications that can arise. A high index of suspicion is necessary for patients with persistent respiratory symptoms following cholecystectomy, and timely imaging and surgical intervention are crucial to minimize morbidity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


