HIV-1 cross-resistance to second-generation non-nucleoside reverse transcriptase inhibitors among individuals failing antiretroviral therapy in Cameroon: implications for the use of long-acting treatment regimens in low- and middle-income countries.
{"title":"HIV-1 cross-resistance to second-generation non-nucleoside reverse transcriptase inhibitors among individuals failing antiretroviral therapy in Cameroon: implications for the use of long-acting treatment regimens in low- and middle-income countries.","authors":"Davy-Hyacinthe Gouissi Anguechia, Yagai Bouba, Ezechiel Ngoufack Jagni Semengue, Desire Takou, Collins Ambe Chenwi, Vincent Kamaël Mekel, Grace Angong Beloumou, Alex Durand Nka, Aude Christelle Ka'e, Sandrine Claire Ndjeyep Djupsa, Vittorio Colizzi, Nicaise Ndembi, Alexis Ndjolo, Dora Mbanya, Carlo-Federico Perno, Joseph Fokam","doi":"10.1093/jacamr/dlaf059","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Several long-acting antiretroviral treatment regimens contain second-generation non-nucleoside reverse transcriptase inhibitors (2ndGenNNRTI). As first-generation NNRTIs (1stGenNNRTI) exhibit some cross-resistance with 2ndGenNNRTI, we sought to evaluate the rate of acquired cross-resistance to 2ndGenNNRTI and its determinants at treatment failure in a typical low- and middle-income country (LMIC) such as Cameroon.</p><p><strong>Patients and methods: </strong>A facility-based cross-sectional study was conducted among patients failing first-/second-line regimens between 2019 and 2023 in Cameroon. HIV-1 Sanger sequencing was performed on plasma and resistance-associated mutations (RAMs) to etravirine, rilpivirine and doravirine were interpreted using HIVdb program v.9.5.0 (HIVdb penalty scores were, ≥60, high resistance; 15-59, intermediate resistance and <15, susceptible) and the IAS-USA 2022 list.</p><p><strong>Results: </strong>Overall, 653 individuals previously exposed to 1stGenNNRTI were enrolled [median (IQR) age 39 (26-46) years and viraemia 59 370 (10 442-244 916) copies/mL]. Importantly, 361 participants were on 1stGenNNRTI-based first-line and 292 on protease inhibitor-based second-line regimen. NNRTIs RAMs were found in up to 90.64% of individuals, with 36.45% having more than three RAMs. Concerning 2ndGenNNRTIs, 77.18% of individuals harboured RAMs conferring high or intermediate-level resistance, with the predicted efficacy of etravirine, doravirine and rilpivirine being 47.17%, 33.23% and 32.31%, respectively. Major 2ndGenNNRTIs RAMs were driven by Y181C (23.74%), K101E (8.57%), Y188L (8.42%) and H221Y (8.42%), while minor RAMs were A98G (18.83%), G190A (18.68%) and P225H (14.70%). A higher prevalence of RAMs was observed in those failing first-line versus second line (81.71% versus 71.57%, respectively, <i>P</i> < 0.001), driven predominantly by the difference in doravirine-RAMs [first line (72.85%) versus second line (59.58%), <i>P</i> < 0.001].</p><p><strong>Conclusions: </strong>Among patients failing treatment in Cameroon, there is a high-level of cross-resistance to 2ndGenNNRTI due to wide exposure to 1stGenNNRTI. Thus, in LMICs sharing similar programmatic features, the use of NNRTI-sparing regimens should be prioritized as a public health approach, while second-generation-NNRTI long-acting regimens should be guided by genotyping or for clients without previous exposure to NNRTIs.</p>","PeriodicalId":14594,"journal":{"name":"JAC-Antimicrobial Resistance","volume":"7 2","pages":"dlaf059"},"PeriodicalIF":3.3000,"publicationDate":"2025-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12034458/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAC-Antimicrobial Resistance","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jacamr/dlaf059","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Several long-acting antiretroviral treatment regimens contain second-generation non-nucleoside reverse transcriptase inhibitors (2ndGenNNRTI). As first-generation NNRTIs (1stGenNNRTI) exhibit some cross-resistance with 2ndGenNNRTI, we sought to evaluate the rate of acquired cross-resistance to 2ndGenNNRTI and its determinants at treatment failure in a typical low- and middle-income country (LMIC) such as Cameroon.
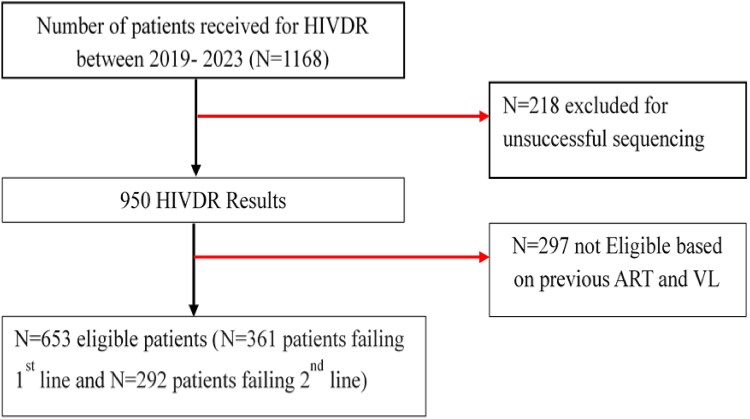
Patients and methods: A facility-based cross-sectional study was conducted among patients failing first-/second-line regimens between 2019 and 2023 in Cameroon. HIV-1 Sanger sequencing was performed on plasma and resistance-associated mutations (RAMs) to etravirine, rilpivirine and doravirine were interpreted using HIVdb program v.9.5.0 (HIVdb penalty scores were, ≥60, high resistance; 15-59, intermediate resistance and <15, susceptible) and the IAS-USA 2022 list.
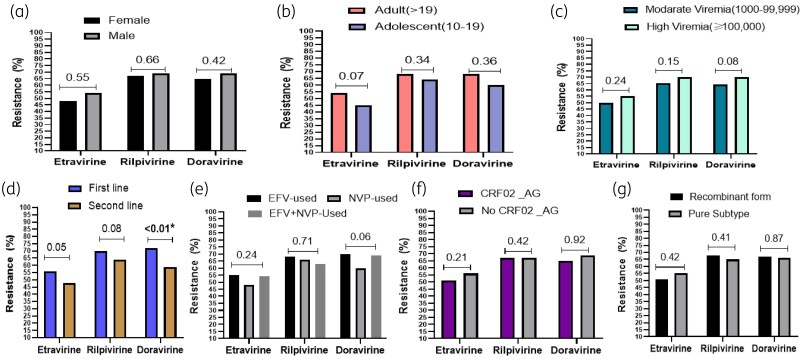
Results: Overall, 653 individuals previously exposed to 1stGenNNRTI were enrolled [median (IQR) age 39 (26-46) years and viraemia 59 370 (10 442-244 916) copies/mL]. Importantly, 361 participants were on 1stGenNNRTI-based first-line and 292 on protease inhibitor-based second-line regimen. NNRTIs RAMs were found in up to 90.64% of individuals, with 36.45% having more than three RAMs. Concerning 2ndGenNNRTIs, 77.18% of individuals harboured RAMs conferring high or intermediate-level resistance, with the predicted efficacy of etravirine, doravirine and rilpivirine being 47.17%, 33.23% and 32.31%, respectively. Major 2ndGenNNRTIs RAMs were driven by Y181C (23.74%), K101E (8.57%), Y188L (8.42%) and H221Y (8.42%), while minor RAMs were A98G (18.83%), G190A (18.68%) and P225H (14.70%). A higher prevalence of RAMs was observed in those failing first-line versus second line (81.71% versus 71.57%, respectively, P < 0.001), driven predominantly by the difference in doravirine-RAMs [first line (72.85%) versus second line (59.58%), P < 0.001].
Conclusions: Among patients failing treatment in Cameroon, there is a high-level of cross-resistance to 2ndGenNNRTI due to wide exposure to 1stGenNNRTI. Thus, in LMICs sharing similar programmatic features, the use of NNRTI-sparing regimens should be prioritized as a public health approach, while second-generation-NNRTI long-acting regimens should be guided by genotyping or for clients without previous exposure to NNRTIs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


