M Senni, E Paoletti, Ewa Stawowczyk, M Hale, A Ramirez de Arellano
{"title":"Economic Evaluation of Patiromer in Patients with Concomitant Heart Failure and Chronic Kidney Disease in Italy.","authors":"M Senni, E Paoletti, Ewa Stawowczyk, M Hale, A Ramirez de Arellano","doi":"10.1007/s41669-025-00581-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hyperkalaemia (HK), in patients with heart failure (HF) with and without chronic kidney disease (CKD), is potentially life-threatening. Risk of HK is further heightened in those patients receiving renin-angiotensin-aldosterone system inhibitors (RAASi), used to reduce cardiovascular morbidity and mortality in HF. Patiromer, an oral potassium (K<sup>+</sup>) binder, has been shown to reduce the risk of HK and enable optimal RAASi dosing. We evaluated the cost-effectiveness of patiromer in HF patients with CKD in the Italian setting, utilising results from the recent DIAMOND clinical trial, which assessed long-term use of patiromer in HK management.</p><p><strong>Methods: </strong>An established Markov model was adapted to include data from DIAMOND using the National Health Service (NHS) perspective. In DIAMOND, patients received patiromer during a run-in period (up to 12 weeks) to achieve optimal RAASi without HK. However, this led to low mean K<sup>+</sup> concentrations in the placebo arm, resulting from a legacy effect of patiromer in the run-in phase of the trial. Therefore, the DIAMOND population was adjusted to a real-world population to better represent the K<sup>+</sup> levels in the standard of care (SoC) arm. Mean K<sup>+</sup> concentration for baseline and the patiromer arm was calculated from the overall population at baseline (screening phase) and after treatment (end of run-in period), respectively. Lifetime trajectories were estimated for quality-adjusted life years (QALYs), life years (LYs) and costs.</p><p><strong>Results: </strong>The economic evaluation model calculated a discounted total average cost per patient of €109,900 for patiromer and €64,847 for SoC. Patiromer generated a gain of 1.97 LYs (1.55 QALYs) compared with SoC. The incremental cost-effectiveness ratio (ICER) for patiromer was €29,060/QALY gained versus SoC.</p><p><strong>Conclusion: </strong>Applying DIAMOND data, patiromer is deemed to be cost-effective at a willingness-to pay threshold of €40,000 per QALY gained in Italy.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"693-706"},"PeriodicalIF":2.1000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12209094/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-025-00581-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hyperkalaemia (HK), in patients with heart failure (HF) with and without chronic kidney disease (CKD), is potentially life-threatening. Risk of HK is further heightened in those patients receiving renin-angiotensin-aldosterone system inhibitors (RAASi), used to reduce cardiovascular morbidity and mortality in HF. Patiromer, an oral potassium (K+) binder, has been shown to reduce the risk of HK and enable optimal RAASi dosing. We evaluated the cost-effectiveness of patiromer in HF patients with CKD in the Italian setting, utilising results from the recent DIAMOND clinical trial, which assessed long-term use of patiromer in HK management.
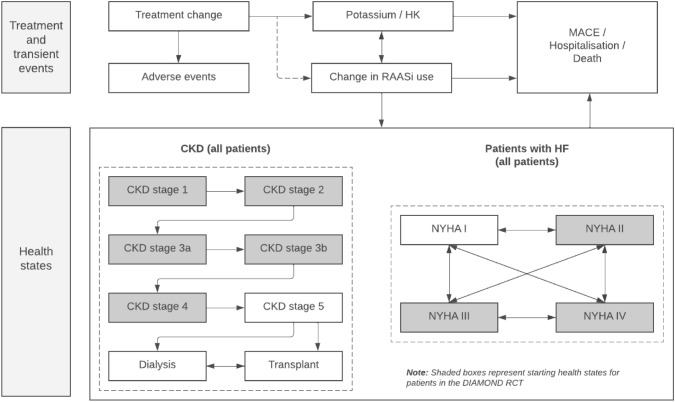
Methods: An established Markov model was adapted to include data from DIAMOND using the National Health Service (NHS) perspective. In DIAMOND, patients received patiromer during a run-in period (up to 12 weeks) to achieve optimal RAASi without HK. However, this led to low mean K+ concentrations in the placebo arm, resulting from a legacy effect of patiromer in the run-in phase of the trial. Therefore, the DIAMOND population was adjusted to a real-world population to better represent the K+ levels in the standard of care (SoC) arm. Mean K+ concentration for baseline and the patiromer arm was calculated from the overall population at baseline (screening phase) and after treatment (end of run-in period), respectively. Lifetime trajectories were estimated for quality-adjusted life years (QALYs), life years (LYs) and costs.
Results: The economic evaluation model calculated a discounted total average cost per patient of €109,900 for patiromer and €64,847 for SoC. Patiromer generated a gain of 1.97 LYs (1.55 QALYs) compared with SoC. The incremental cost-effectiveness ratio (ICER) for patiromer was €29,060/QALY gained versus SoC.
Conclusion: Applying DIAMOND data, patiromer is deemed to be cost-effective at a willingness-to pay threshold of €40,000 per QALY gained in Italy.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


