Angel J Cadena-Tejada, Shaista Alam, Varoon Thavapalan, Sara Habib, Fred Rincon
{"title":"In-hospital Mortality is Lower in Brain-Injured Patients After Admission to a Neuroscience Intensive Care Unit: A Multi-Center Cohort Study.","authors":"Angel J Cadena-Tejada, Shaista Alam, Varoon Thavapalan, Sara Habib, Fred Rincon","doi":"10.1177/08850666251325778","DOIUrl":null,"url":null,"abstract":"<p><p>ObjectiveTo study the impact of dedicated Neuroscience Intensive Care Units (NSU) on clinical outcomes in patients with acute brain injury.DesignRetrospective, multicenter cohort study.Setting172 intensive care units within the United States.PatientsProspectively compiled and maintained a registry of a total of 32,047 brain-injured patients (stroke = AIS, aneurysmal-bleed = SAH, intra-cerebral-hemorrhage = ICH, and traumatic brain injury = TBI) from 2008-2013.MeasurementsExposure of interest was the type of intensive care unit (ICU), divided into NSU and non-NSU (medical = MICU, non-neurosurgical = SICU, trauma = TICU, cardiac = CCU, or mixed). Outcomes of interest were the actual and predicted in-hospital mortality, ICU mortality, ICU length of stay, and ventilator-free days. We calculated the actual and predicted in-hospital mortality using the Cerner Corporation Acute Physiology and Chronic Health Evaluation IV (APACHE Clinical Information System, CIS). We then compared the actual in-hospital mortality against the mortality prediction of the APACHE-IV model based on ICU designation (NSU v. non-NSU). The multivariable model was adjusted for within-hospital effects and known predictors of poor outcomes after brain injury.Main ResultsNational APACHE-IV predicted that in-hospital mortality was higher for NSU admissions than non-NSU admissions (21% v. 19%, p < .0001). However, the actual ICU mortality (10% vs 11%, p < 0.01) and in-hospital mortality (15% vs 16%, p = 0.06) were lower in patients admitted to a NSU as compared to non-NSU. We observed lower ventilator-free days (22 vs 24, p < 0.001) in NSU v. non-NSU. In the multivariable regression analysis adjusted for within-hospital effects, known variables of poor outcome, and the severity of illness APACHE-III score, the in-hospital mortality was lower for NSU admissions (OR, 0.8; 95%CI, 0.7-0.9, p = 0.02) as compared to non-NSU.ConclusionAdmission of critically ill brain-injured patients to dedicated NSUs is associated with lower actual in-hospital mortality. Future iterations of APACHE-IV modeling may need to incorporate NSU designations for calculations of expected mortality among brain-injured patients.</p>","PeriodicalId":16307,"journal":{"name":"Journal of Intensive Care Medicine","volume":" ","pages":"902-906"},"PeriodicalIF":2.1000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12177187/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/08850666251325778","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
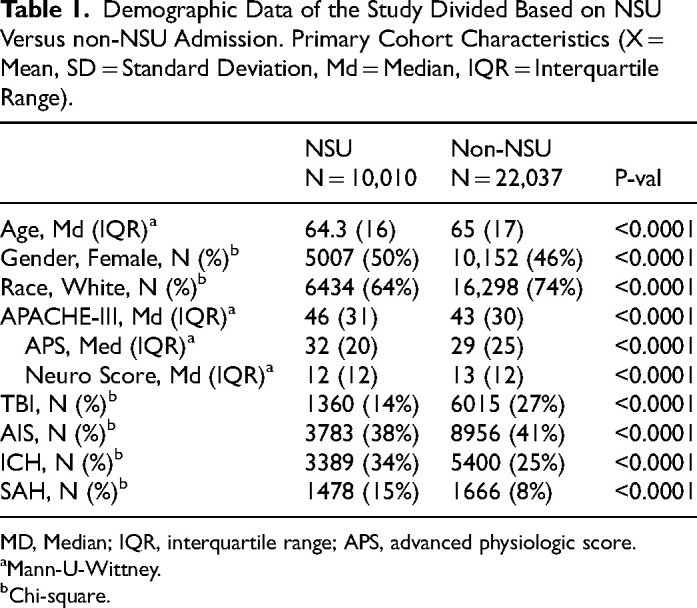
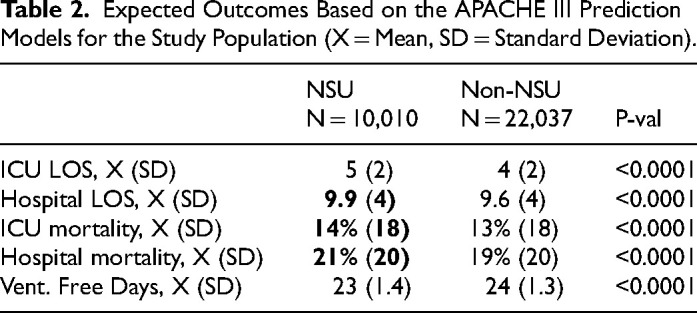
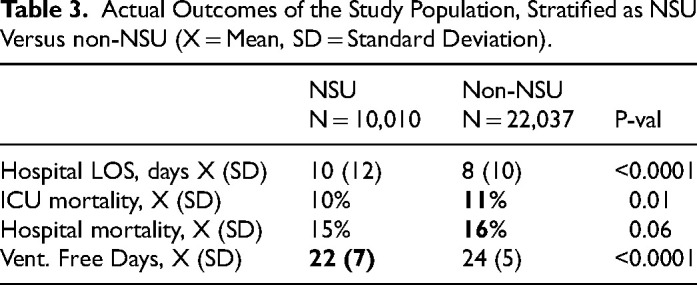
ObjectiveTo study the impact of dedicated Neuroscience Intensive Care Units (NSU) on clinical outcomes in patients with acute brain injury.DesignRetrospective, multicenter cohort study.Setting172 intensive care units within the United States.PatientsProspectively compiled and maintained a registry of a total of 32,047 brain-injured patients (stroke = AIS, aneurysmal-bleed = SAH, intra-cerebral-hemorrhage = ICH, and traumatic brain injury = TBI) from 2008-2013.MeasurementsExposure of interest was the type of intensive care unit (ICU), divided into NSU and non-NSU (medical = MICU, non-neurosurgical = SICU, trauma = TICU, cardiac = CCU, or mixed). Outcomes of interest were the actual and predicted in-hospital mortality, ICU mortality, ICU length of stay, and ventilator-free days. We calculated the actual and predicted in-hospital mortality using the Cerner Corporation Acute Physiology and Chronic Health Evaluation IV (APACHE Clinical Information System, CIS). We then compared the actual in-hospital mortality against the mortality prediction of the APACHE-IV model based on ICU designation (NSU v. non-NSU). The multivariable model was adjusted for within-hospital effects and known predictors of poor outcomes after brain injury.Main ResultsNational APACHE-IV predicted that in-hospital mortality was higher for NSU admissions than non-NSU admissions (21% v. 19%, p < .0001). However, the actual ICU mortality (10% vs 11%, p < 0.01) and in-hospital mortality (15% vs 16%, p = 0.06) were lower in patients admitted to a NSU as compared to non-NSU. We observed lower ventilator-free days (22 vs 24, p < 0.001) in NSU v. non-NSU. In the multivariable regression analysis adjusted for within-hospital effects, known variables of poor outcome, and the severity of illness APACHE-III score, the in-hospital mortality was lower for NSU admissions (OR, 0.8; 95%CI, 0.7-0.9, p = 0.02) as compared to non-NSU.ConclusionAdmission of critically ill brain-injured patients to dedicated NSUs is associated with lower actual in-hospital mortality. Future iterations of APACHE-IV modeling may need to incorporate NSU designations for calculations of expected mortality among brain-injured patients.
期刊介绍:
Journal of Intensive Care Medicine (JIC) is a peer-reviewed bi-monthly journal offering medical and surgical clinicians in adult and pediatric intensive care state-of-the-art, broad-based analytic reviews and updates, original articles, reports of large clinical series, techniques and procedures, topic-specific electronic resources, book reviews, and editorials on all aspects of intensive/critical/coronary care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


