{"title":"Comparative Evaluation of Risk of Death in Mechanically Ventilated Patients With COVID-19 and Influenza: A Population-Based Cohort Study.","authors":"Lavi Oud, John Garza","doi":"10.14740/jocmr6189","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Reports on the comparative mortality among mechanically ventilated patients with coronavirus disease 2019 (COVID-19) and influenza show conflicting findings, but studies focused largely on the early phase of the pandemic, using historical influenza comparators. We sought to examine the population-level comparative mortality among mechanically ventilated patients with COVID-19 during the latter pandemic years using contemporaneous influenza comparators.</p><p><strong>Methods: </strong>We used a statewide dataset to identify mechanically ventilated hospitalizations aged ≥ 18 years with COVID-19 or influenza in Texas between October 2021 and March 2023. Their comparative short-term mortality (in-hospital death or discharge to hospice) was estimated using overlap propensity score weighting (primary model), entropy balance, and hierarchical logistic models.</p><p><strong>Results: </strong>Among 22,195 mechanically ventilated hospitalizations, 19,659 (88.6%) had COVID-19 and 2,536 (11.4%) had influenza. Compared to mechanically ventilated hospitalizations with influenza, those with COVID-19 were more commonly racial or ethnic minority (49.3% vs. 48.4%) and had lower mean (standard deviation (SD)) Deyo comorbidity index (2.04 (2.03) vs. 2.53 (1.91)), but higher number of organ dysfunctions (2.60 (1.37) vs. 2.13 (1.27)), respectively. Short-term mortality among mechanically ventilated hospitalizations with COVID-19 and influenza was 49.1% vs. 20.7%. The risk of short-term mortality was attenuated but remained higher among hospitalizations with COVID-19 in the primary model (adjusted risk ratio: 1.24 (95% confidence interval (CI): 1.18 - 1.30); adjusted risk difference 8.8% (95% CI: 6.7 - 10.4)), with consistent findings in alternative models, subgroups, and sensitivity analyses.</p><p><strong>Conclusions: </strong>Population-level short-term mortality among mechanically ventilated hospitalizations with COVID-19 has been higher than that among those with influenza during the latter years of the pandemic.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"17 4","pages":"187-199"},"PeriodicalIF":2.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12045779/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr6189","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Reports on the comparative mortality among mechanically ventilated patients with coronavirus disease 2019 (COVID-19) and influenza show conflicting findings, but studies focused largely on the early phase of the pandemic, using historical influenza comparators. We sought to examine the population-level comparative mortality among mechanically ventilated patients with COVID-19 during the latter pandemic years using contemporaneous influenza comparators.
Methods: We used a statewide dataset to identify mechanically ventilated hospitalizations aged ≥ 18 years with COVID-19 or influenza in Texas between October 2021 and March 2023. Their comparative short-term mortality (in-hospital death or discharge to hospice) was estimated using overlap propensity score weighting (primary model), entropy balance, and hierarchical logistic models.
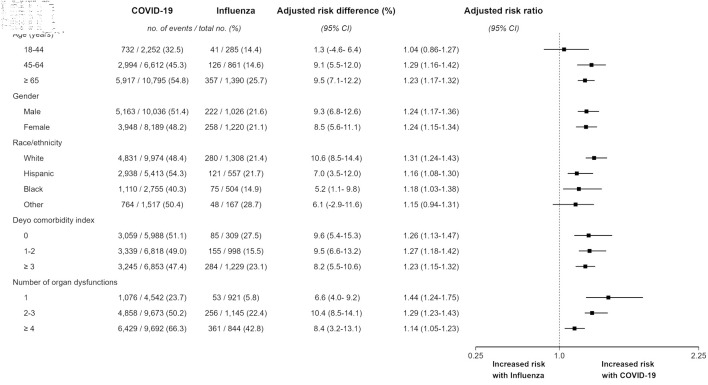
Results: Among 22,195 mechanically ventilated hospitalizations, 19,659 (88.6%) had COVID-19 and 2,536 (11.4%) had influenza. Compared to mechanically ventilated hospitalizations with influenza, those with COVID-19 were more commonly racial or ethnic minority (49.3% vs. 48.4%) and had lower mean (standard deviation (SD)) Deyo comorbidity index (2.04 (2.03) vs. 2.53 (1.91)), but higher number of organ dysfunctions (2.60 (1.37) vs. 2.13 (1.27)), respectively. Short-term mortality among mechanically ventilated hospitalizations with COVID-19 and influenza was 49.1% vs. 20.7%. The risk of short-term mortality was attenuated but remained higher among hospitalizations with COVID-19 in the primary model (adjusted risk ratio: 1.24 (95% confidence interval (CI): 1.18 - 1.30); adjusted risk difference 8.8% (95% CI: 6.7 - 10.4)), with consistent findings in alternative models, subgroups, and sensitivity analyses.
Conclusions: Population-level short-term mortality among mechanically ventilated hospitalizations with COVID-19 has been higher than that among those with influenza during the latter years of the pandemic.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


