Anesthetic management of coronary artery reconstruction in a patient with myocardial ischemia caused by an anomalous origin of the right coronary artery running between the great vessels: a case report.
{"title":"Anesthetic management of coronary artery reconstruction in a patient with myocardial ischemia caused by an anomalous origin of the right coronary artery running between the great vessels: a case report.","authors":"Riki Kuzuno, Shuji Kawamoto, Kenichiro Tatsumi, Chikashi Takeda, Moritoki Egi","doi":"10.1186/s40981-025-00786-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronary artery origin anomalies, though often incidentally detected, can lead to sudden death. Comprehensive perioperative management is essential. We report a case of an anomalous right coronary artery (RCA) arising from the left main coronary artery (LMCA) and coursing between the aorta and pulmonary artery, discovered after myocardial infarction, in which intraoperative management ensured successful coronary reconstruction.</p><p><strong>Case presentation: </strong>A 49-year-old woman presented with chest pain and ST segment elevation. Coronary angiography revealed an anomalous RCA demonstrating compressive ischemia by the aorta and pulmonary artery. Preoperatively, blood pressure was stabilized with an isosorbide dinitrate patch. Under cardiopulmonary bypass, the RCA was transected and reanastomosed to its physiological aortic position. Intraoperatively, nicorandil was administered to suppress vascular smooth muscle contraction, while five-lead ECG, transesophageal echocardiography, and operative ultrasound monitoring enabled early detection of ischemia and prevented hypertension. Postoperative ventricular premature contractions resolved by the next day, with uneventful recovery.</p><p><strong>Conclusions: </strong>Targeted pharmacologic blood pressure control and multimodal monitoring are vital for safe perioperative outcomes in anomalous coronary artery origin cases.</p>","PeriodicalId":14635,"journal":{"name":"JA Clinical Reports","volume":"11 1","pages":"21"},"PeriodicalIF":1.0000,"publicationDate":"2025-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12006570/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JA Clinical Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40981-025-00786-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
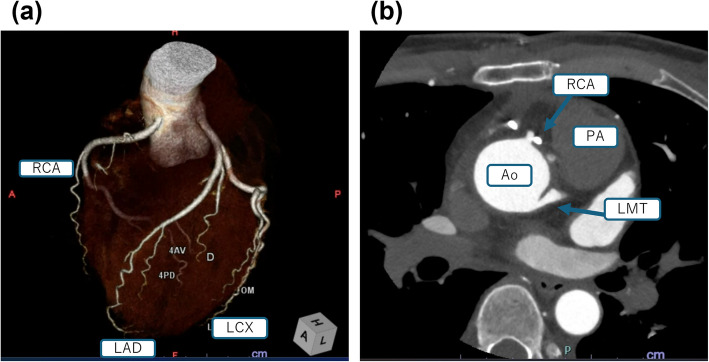
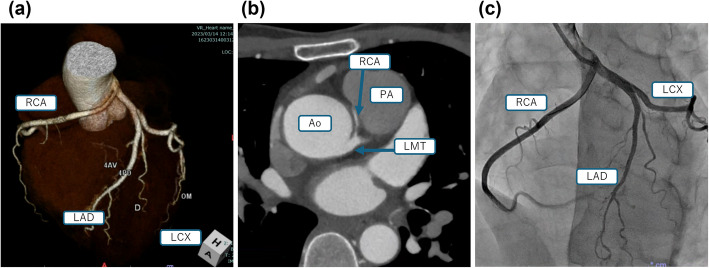
Background: Coronary artery origin anomalies, though often incidentally detected, can lead to sudden death. Comprehensive perioperative management is essential. We report a case of an anomalous right coronary artery (RCA) arising from the left main coronary artery (LMCA) and coursing between the aorta and pulmonary artery, discovered after myocardial infarction, in which intraoperative management ensured successful coronary reconstruction.
Case presentation: A 49-year-old woman presented with chest pain and ST segment elevation. Coronary angiography revealed an anomalous RCA demonstrating compressive ischemia by the aorta and pulmonary artery. Preoperatively, blood pressure was stabilized with an isosorbide dinitrate patch. Under cardiopulmonary bypass, the RCA was transected and reanastomosed to its physiological aortic position. Intraoperatively, nicorandil was administered to suppress vascular smooth muscle contraction, while five-lead ECG, transesophageal echocardiography, and operative ultrasound monitoring enabled early detection of ischemia and prevented hypertension. Postoperative ventricular premature contractions resolved by the next day, with uneventful recovery.
Conclusions: Targeted pharmacologic blood pressure control and multimodal monitoring are vital for safe perioperative outcomes in anomalous coronary artery origin cases.
期刊介绍:
JA Clinical Reports is a companion journal to the Journal of Anesthesia (JA), the official journal of the Japanese Society of Anesthesiologists (JSA). This journal is an open access, peer-reviewed, online journal related to clinical anesthesia practices such as anesthesia management, pain management and intensive care. Case reports are very important articles from the viewpoint of education and the cultivation of scientific thinking in the field of anesthesia. However, submissions of anesthesia research and clinical reports from Japan are notably decreasing in major anesthesia journals. Therefore, the JSA has decided to launch a new journal, JA Clinical Reports, to encourage JSA members, particularly junior Japanese anesthesiologists, to publish papers in English language.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


