{"title":"Acute Ischemic and Hemorrhagic Cerebrovascular Strokes After Cardiac Surgery: Incidence, Predictors, and Outcomes.","authors":"Mohamed Laimoud, Mosleh Nazzal Alanazi, Patricia Machado, Mary Jane Maghirang, Suha Althibait, Shatha Al-Mutlaq, Munirah Alomran, Imad Bou-Saad, Lamees Subhi, Reem Almutairi, Renad Nadhreen, Hamza Busaleh, Sreedevi Pillai, Saranya Sidharthan, Tareq Almazeedi, Zohair Al-Halees","doi":"10.1155/ccrp/6645363","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Many studies have attempted to determine the incidence, predictors, and outcomes of cerebrovascular stroke after cardiac surgery, with different, sometimes contradictory, results because of differences in population risk profiles, study design, and surgical details. <b>Methods:</b> We retrospectively reviewed the records of all adult patients who underwent cardiac surgery between January 2018 and January 2023. Univariate, multivariable, and survival analyses were performed to identify the outcomes and predictors of ischemic and hemorrhagic strokes. <b>Results:</b> Of the 1334 patients studied, 70 (5.2%) patients had ischemic stroke, 23 (1.7%) had intracranial hemorrhage (ICH), and 9 (0.7%) had combined ischemic and hemorrhagic strokes. The patients who developed strokes had longer cardiopulmonary bypass (CPB) time (165.5 [126, 234] versus 136 [104, 171] min, <i>p</i> < 0.001) and aortic cross-clamping time (112 [79, 163] versus 89 [75, 121.5] min, <i>p</i> < 0.001), with higher rates of intra-aortic balloon pump (IABP) use (13.3% vs. 4.4%, <i>p</i> < 0.001), veno-arterial extracorporeal membrane oxygenation use (24.8% vs. 12.37%, <i>p</i> < 0.001), and mediastinal exploration for bleeding (22.9% vs. 8.9%, <i>p</i> < 0.0011). The patients who developed strokes showed increased hospital mortality (37.1% vs. 5.6%, <i>p</i> < 0.001), new need for dialysis (29.5% vs. 10.7%, <i>p</i> < 0.001), higher rate of tracheostomy (13.3% vs. 1.2%, <i>p</i> < 0.001), and longer intensive care unit (ICU) stay (12 [7, 28] versus 3 [2, 8] days, <i>p</i> < 0.001) and post-ICU stay (16 [7, 39] versus 5 [3, 10] days, <i>p</i> < 0.001). Follow-up for 36.4 (21.67, 50.7) months revealed an insignificant mortality difference, but there was an increased risk of recurrent cerebrovascular strokes. Cox-proportional hazards regression showed an increased risk of hospital mortality after cardiac surgery in patients who developed acute ischemic stroke (HR: 5.075, 95% CI: 3.28-7.851, <i>p</i> < 0.001) and ICH (HR: 12.288, 95% CI: 7.576-19.93, <i>p</i> < 0.001). Logistic multivariable regression showed that increased age, hyperlactatemia, redo cardiotomy, history of old stroke, CPB time, and perioperative IABP use were the predictors of ischemic stroke. Young age, old ICH, hyperlactatemia, and hypoalbuminemia were the predictors of postoperative ICH. Postoperative ICH, ischemic stroke, atrial fibrillation, chronic kidney disease, blood lactate level 24 h after surgery, and increased age were the independent predictors of mortality. <b>Conclusions:</b> Ischemic and hemorrhagic cerebrovascular strokes are serious complications that increase postoperative mortality and prolong hospitalization after cardiac surgery. Atrial fibrillation was not a significant predictor of postoperative stroke but was a predictor of hospital mortality. Careful attention should be given to maintaining hemodynamic stability and minimizing CPB time, especially in patients with a history of cerebrovascular strokes and redo cardiotomy.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2025 ","pages":"6645363"},"PeriodicalIF":1.8000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058317/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/ccrp/6645363","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
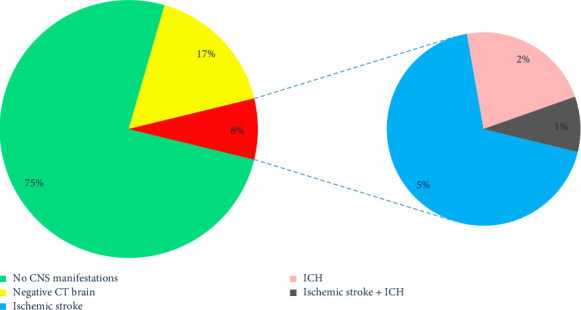
Background: Many studies have attempted to determine the incidence, predictors, and outcomes of cerebrovascular stroke after cardiac surgery, with different, sometimes contradictory, results because of differences in population risk profiles, study design, and surgical details. Methods: We retrospectively reviewed the records of all adult patients who underwent cardiac surgery between January 2018 and January 2023. Univariate, multivariable, and survival analyses were performed to identify the outcomes and predictors of ischemic and hemorrhagic strokes. Results: Of the 1334 patients studied, 70 (5.2%) patients had ischemic stroke, 23 (1.7%) had intracranial hemorrhage (ICH), and 9 (0.7%) had combined ischemic and hemorrhagic strokes. The patients who developed strokes had longer cardiopulmonary bypass (CPB) time (165.5 [126, 234] versus 136 [104, 171] min, p < 0.001) and aortic cross-clamping time (112 [79, 163] versus 89 [75, 121.5] min, p < 0.001), with higher rates of intra-aortic balloon pump (IABP) use (13.3% vs. 4.4%, p < 0.001), veno-arterial extracorporeal membrane oxygenation use (24.8% vs. 12.37%, p < 0.001), and mediastinal exploration for bleeding (22.9% vs. 8.9%, p < 0.0011). The patients who developed strokes showed increased hospital mortality (37.1% vs. 5.6%, p < 0.001), new need for dialysis (29.5% vs. 10.7%, p < 0.001), higher rate of tracheostomy (13.3% vs. 1.2%, p < 0.001), and longer intensive care unit (ICU) stay (12 [7, 28] versus 3 [2, 8] days, p < 0.001) and post-ICU stay (16 [7, 39] versus 5 [3, 10] days, p < 0.001). Follow-up for 36.4 (21.67, 50.7) months revealed an insignificant mortality difference, but there was an increased risk of recurrent cerebrovascular strokes. Cox-proportional hazards regression showed an increased risk of hospital mortality after cardiac surgery in patients who developed acute ischemic stroke (HR: 5.075, 95% CI: 3.28-7.851, p < 0.001) and ICH (HR: 12.288, 95% CI: 7.576-19.93, p < 0.001). Logistic multivariable regression showed that increased age, hyperlactatemia, redo cardiotomy, history of old stroke, CPB time, and perioperative IABP use were the predictors of ischemic stroke. Young age, old ICH, hyperlactatemia, and hypoalbuminemia were the predictors of postoperative ICH. Postoperative ICH, ischemic stroke, atrial fibrillation, chronic kidney disease, blood lactate level 24 h after surgery, and increased age were the independent predictors of mortality. Conclusions: Ischemic and hemorrhagic cerebrovascular strokes are serious complications that increase postoperative mortality and prolong hospitalization after cardiac surgery. Atrial fibrillation was not a significant predictor of postoperative stroke but was a predictor of hospital mortality. Careful attention should be given to maintaining hemodynamic stability and minimizing CPB time, especially in patients with a history of cerebrovascular strokes and redo cardiotomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


