Yue Guo, Jin Niu, Natalia A Quijano Cardé, Liviawati Wu, Xin Miao, Shalla Hanson, Yaming Su, Carlos Pérez Ruixo, Deeksha Vishwamitra, Katherine Chastain, Mahesh N Samtani, Weirong Wang, Nahor Haddish-Berhane
{"title":"Teclistamab Dosing in Responders: Modeling and Simulation Results from the MajesTEC-1 Study in Relapsed/Refractory Multiple Myeloma.","authors":"Yue Guo, Jin Niu, Natalia A Quijano Cardé, Liviawati Wu, Xin Miao, Shalla Hanson, Yaming Su, Carlos Pérez Ruixo, Deeksha Vishwamitra, Katherine Chastain, Mahesh N Samtani, Weirong Wang, Nahor Haddish-Berhane","doi":"10.1007/s11523-025-01149-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Based on the phase I/II MajesTEC-1 study, the B-cell maturation antigen (BCMA) and cluster of differentiation (CD)3 bispecific antibody, teclistamab, is approved for relapsed/refractory multiple myeloma (RRMM) at a dose of 1.5 mg/kg weekly (QW), with the option to switch to 1.5 mg/kg every other week (Q2W) in patients maintaining complete response (CR) or better for ≥ 6 months on the QW schedule.</p><p><strong>Objective: </strong>We report the pharmacokinetics (PK), pharmacodynamics, and anticancer activity of teclistamab 1.5 mg/kg Q2W, and the PK of teclistamab 3 mg/kg every 4 weeks (Q4W), on the basis of modeling and simulation results from MajesTEC-1.</p><p><strong>Methods: </strong>Teclistamab PK was assessed using a population PK approach. Exposure-response analysis was based on individual estimated teclistamab serum trough concentration (C<sub>trough</sub>). The impact of responders switching to Q2W teclistamab dosing on the formation of the key pharmacological species that drive the mechanism of action of teclistamab (i.e., the trimer formed by simultaneous engagement of teclistamab with BCMA on target multiple myeloma cells and CD3 on effector T cells) was estimated using a quantitative systems pharmacology (QSP) model. Additionally, steady-state teclistamab PK and trimer was simulated for the 1.5 mg/kg Q2W and Q4W (3 mg/kg or 1.5 mg/kg) doses.</p><p><strong>Results: </strong>Median estimated teclistamab serum C<sub>trough</sub> was lower after the first and fourth Q2W doses (14.4 and 11.7 µg/mL, respectively) than after QW doses (20.4 µg/mL) but remained above the 90% maximal effective concentration. No statistically significant exposure-response trend was observed for duration of response (DOR), progression-free survival, or overall survival in responders who switched to teclistamab 1.5 mg/kg Q2W dosing. Despite the lower teclistamab serum C<sub>trough</sub>, the QSP model estimated comparable target cell-biologics-effector cell (TBE) trimer formation, tumor volume reduction, and DOR for responders switching to 1.5 mg/kg Q2W dosing versus not switching. Steady-state exposure metrics and trimer formation with teclistamab 3 mg/kg Q4W were estimated to be comparable with those at 1.5 mg/kg Q2W.</p><p><strong>Conclusions: </strong>MajesTEC-1 modeling and simulation results, which contributed to the teclistamab label update, support the approved switch to teclistamab 1.5 mg/kg Q2W in patients maintaining ≥ CR for ≥ 6 months on the QW dose, without negatively impacting clinical efficacy. In addition, it is estimated that the 3 mg/kg Q4W schedule will provide maintenance of response comparable with the 1.5 mg/kg Q2W schedule. Teclistamab 3 mg/kg Q4W dosing will be evaluated in > 800 patients in three phase III studies in early line RRMM (MajesTEC-3, MajesTEC-9, and MonumenTAL-6) and in 100 patients in RRMM in the phase I MajesTEC-10 study.</p><p><strong>Clinical trial registration: </strong>NCT03145181 (phase I, 9 May 2017); NCT04557098 (phase II, 21 September 2020).</p>","PeriodicalId":22195,"journal":{"name":"Targeted Oncology","volume":" ","pages":"651-661"},"PeriodicalIF":4.0000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12307566/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Targeted Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11523-025-01149-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Based on the phase I/II MajesTEC-1 study, the B-cell maturation antigen (BCMA) and cluster of differentiation (CD)3 bispecific antibody, teclistamab, is approved for relapsed/refractory multiple myeloma (RRMM) at a dose of 1.5 mg/kg weekly (QW), with the option to switch to 1.5 mg/kg every other week (Q2W) in patients maintaining complete response (CR) or better for ≥ 6 months on the QW schedule.
Objective: We report the pharmacokinetics (PK), pharmacodynamics, and anticancer activity of teclistamab 1.5 mg/kg Q2W, and the PK of teclistamab 3 mg/kg every 4 weeks (Q4W), on the basis of modeling and simulation results from MajesTEC-1.
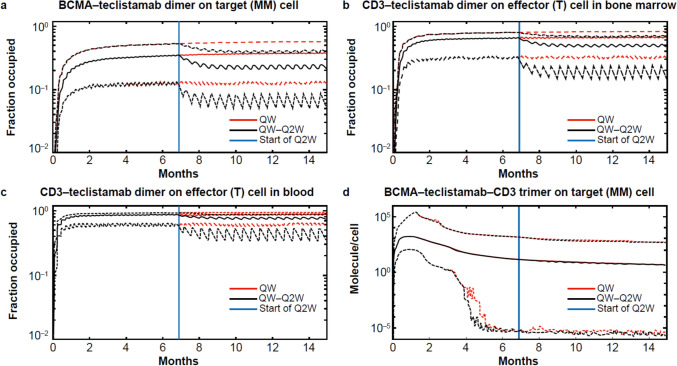
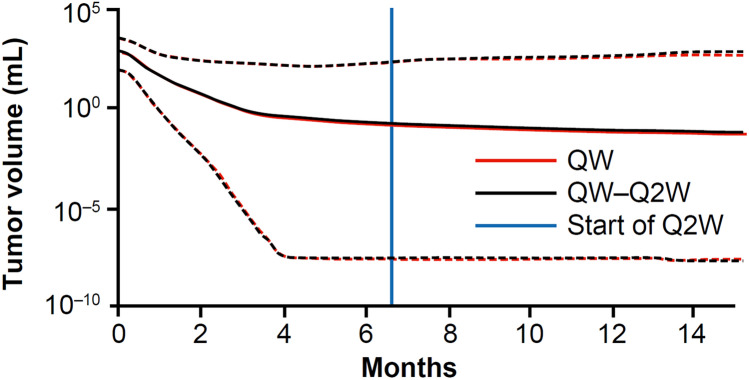
Methods: Teclistamab PK was assessed using a population PK approach. Exposure-response analysis was based on individual estimated teclistamab serum trough concentration (Ctrough). The impact of responders switching to Q2W teclistamab dosing on the formation of the key pharmacological species that drive the mechanism of action of teclistamab (i.e., the trimer formed by simultaneous engagement of teclistamab with BCMA on target multiple myeloma cells and CD3 on effector T cells) was estimated using a quantitative systems pharmacology (QSP) model. Additionally, steady-state teclistamab PK and trimer was simulated for the 1.5 mg/kg Q2W and Q4W (3 mg/kg or 1.5 mg/kg) doses.
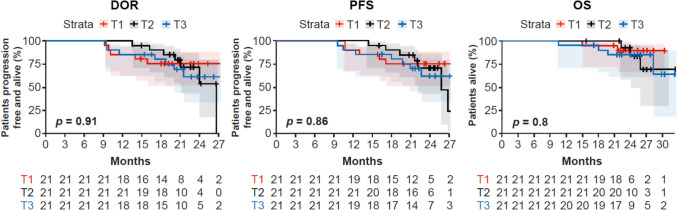
Results: Median estimated teclistamab serum Ctrough was lower after the first and fourth Q2W doses (14.4 and 11.7 µg/mL, respectively) than after QW doses (20.4 µg/mL) but remained above the 90% maximal effective concentration. No statistically significant exposure-response trend was observed for duration of response (DOR), progression-free survival, or overall survival in responders who switched to teclistamab 1.5 mg/kg Q2W dosing. Despite the lower teclistamab serum Ctrough, the QSP model estimated comparable target cell-biologics-effector cell (TBE) trimer formation, tumor volume reduction, and DOR for responders switching to 1.5 mg/kg Q2W dosing versus not switching. Steady-state exposure metrics and trimer formation with teclistamab 3 mg/kg Q4W were estimated to be comparable with those at 1.5 mg/kg Q2W.
Conclusions: MajesTEC-1 modeling and simulation results, which contributed to the teclistamab label update, support the approved switch to teclistamab 1.5 mg/kg Q2W in patients maintaining ≥ CR for ≥ 6 months on the QW dose, without negatively impacting clinical efficacy. In addition, it is estimated that the 3 mg/kg Q4W schedule will provide maintenance of response comparable with the 1.5 mg/kg Q2W schedule. Teclistamab 3 mg/kg Q4W dosing will be evaluated in > 800 patients in three phase III studies in early line RRMM (MajesTEC-3, MajesTEC-9, and MonumenTAL-6) and in 100 patients in RRMM in the phase I MajesTEC-10 study.
Clinical trial registration: NCT03145181 (phase I, 9 May 2017); NCT04557098 (phase II, 21 September 2020).
期刊介绍:
Targeted Oncology addresses physicians and scientists committed to oncology and cancer research by providing a programme of articles on molecularly targeted pharmacotherapy in oncology. The journal includes:
Original Research Articles on all aspects of molecularly targeted agents for the treatment of cancer, including immune checkpoint inhibitors and related approaches.
Comprehensive narrative Review Articles and shorter Leading Articles discussing relevant clinically established as well as emerging agents and pathways.
Current Opinion articles that place interesting areas in perspective.
Therapy in Practice articles that provide a guide to the optimum management of a condition and highlight practical, clinically relevant considerations and recommendations.
Systematic Reviews that use explicit, systematic methods as outlined by the PRISMA statement.
Adis Drug Reviews of the properties and place in therapy of both newer and established targeted drugs in oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


