Nasima Mohamed Elkenany, Zia Ul Sabah, Nadia Ahmed Agiba, Hanaa Kamel Elmahdy, Eman Aziz Yousef Elsherbiny, Salwa Rashad Aly Said, Eman Mostafa Nassef, Ahmed Mohamed Ewis Alhawy, Marwan Sayed Mohamed Ahmed, Ashraf Mohammed Said Elsharkawy, Amr Mahmoud Mohamed Hussein, Abeer Ahmed Elmalah
{"title":"Association of Prognostic Nutritional Index with Post-Discharge Bleeding After Percutaneous Coronary Intervention in ACS Patients on DAPT.","authors":"Nasima Mohamed Elkenany, Zia Ul Sabah, Nadia Ahmed Agiba, Hanaa Kamel Elmahdy, Eman Aziz Yousef Elsherbiny, Salwa Rashad Aly Said, Eman Mostafa Nassef, Ahmed Mohamed Ewis Alhawy, Marwan Sayed Mohamed Ahmed, Ashraf Mohammed Said Elsharkawy, Amr Mahmoud Mohamed Hussein, Abeer Ahmed Elmalah","doi":"10.2147/TCRM.S496656","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Malnutrition increases bleeding risk by reducing thrombogenicity, impairing platelet aggregation, prolonging bleeding time, and promoting systemic inflammation, which affects vascular permeability and angiogenesis. The Prognostic Nutritional Index (PNI), calculated from serum albumin and lymphocyte count, reflects both nutritional and inflammatory status. This study aimed to assess PNI's association with bleeding risk in acute coronary syndrome (ACS) patients on dual antiplatelet therapy (DAPT).</p><p><strong>Patients and methods: </strong>This prospective, single-center observational cohort study enrolled 1843 patients presenting with acute coronary syndrome (ACS) who underwent percutaneous coronary intervention (PCI). ROC analysis determined 42.7 as the optimal PNI cut-off value for risk stratification. Participants were stratified into distinct groups based on Prognostic Nutritional Index (PNI) cut-off values, a composite marker derived from serum albumin levels and peripheral lymphocyte counts, reflecting both nutritional and inflammatory status. Patients were prospectively followed for 12 months post-discharge to assess the occurrence of actionable bleeding events, with the aim of evaluating the association between PNI and post-PCI bleeding risk.</p><p><strong>Results: </strong>The study cohort had a mean age of 66.4, with 65.16% male. After PCI, 98.04% were on DAPT. Patients were divided into Group I (PNI ≥ 42.7, n = 1290) and Group II (PNI < 42.7, n = 553). During follow-up, 5.58% of patients experienced actionable bleeding, with 3.5% in Group I and 10.3% in Group II (p < 0.0001). Multivariable Cox regression analysis revealed that PNI < 42.7 was a significant independent predictor of bleeding (HR: 1.7; 95% CI: 1.1-2.5; p < 0.003).</p><p><strong>Conclusion: </strong>Baseline PNI is an independent predictor of post-discharge bleeding in ACS patients on DAPT after PCI, suggesting it could be a valuable tool for risk stratification of bleeding in these patients.</p>","PeriodicalId":22977,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"21 ","pages":"455-466"},"PeriodicalIF":2.8000,"publicationDate":"2025-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11995920/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S496656","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Malnutrition increases bleeding risk by reducing thrombogenicity, impairing platelet aggregation, prolonging bleeding time, and promoting systemic inflammation, which affects vascular permeability and angiogenesis. The Prognostic Nutritional Index (PNI), calculated from serum albumin and lymphocyte count, reflects both nutritional and inflammatory status. This study aimed to assess PNI's association with bleeding risk in acute coronary syndrome (ACS) patients on dual antiplatelet therapy (DAPT).
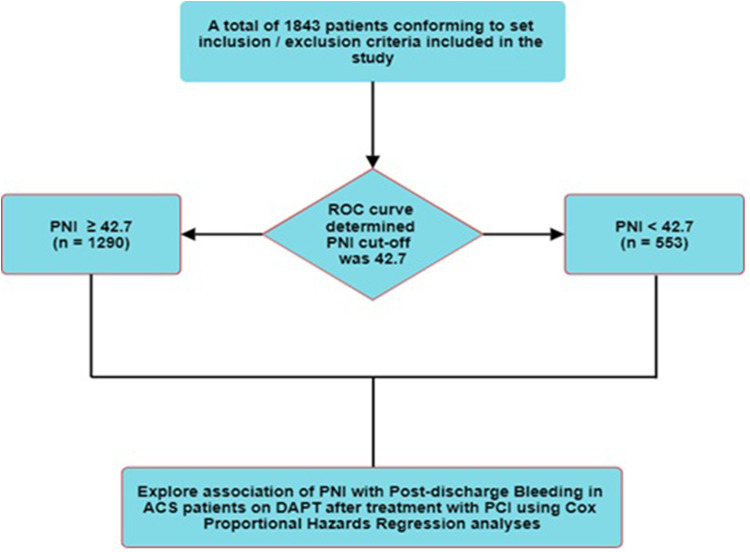
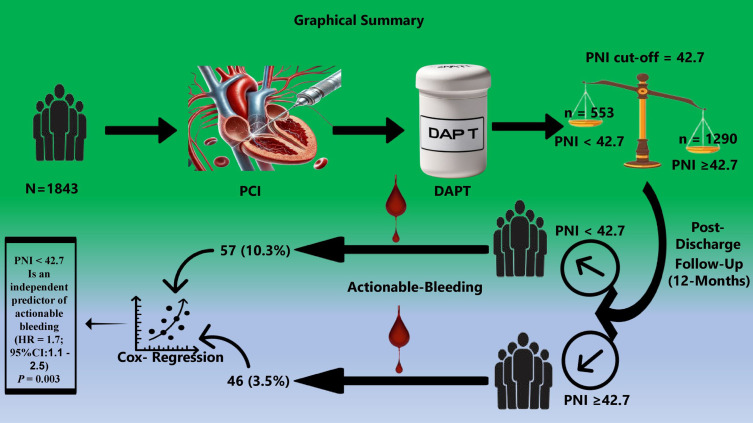
Patients and methods: This prospective, single-center observational cohort study enrolled 1843 patients presenting with acute coronary syndrome (ACS) who underwent percutaneous coronary intervention (PCI). ROC analysis determined 42.7 as the optimal PNI cut-off value for risk stratification. Participants were stratified into distinct groups based on Prognostic Nutritional Index (PNI) cut-off values, a composite marker derived from serum albumin levels and peripheral lymphocyte counts, reflecting both nutritional and inflammatory status. Patients were prospectively followed for 12 months post-discharge to assess the occurrence of actionable bleeding events, with the aim of evaluating the association between PNI and post-PCI bleeding risk.
Results: The study cohort had a mean age of 66.4, with 65.16% male. After PCI, 98.04% were on DAPT. Patients were divided into Group I (PNI ≥ 42.7, n = 1290) and Group II (PNI < 42.7, n = 553). During follow-up, 5.58% of patients experienced actionable bleeding, with 3.5% in Group I and 10.3% in Group II (p < 0.0001). Multivariable Cox regression analysis revealed that PNI < 42.7 was a significant independent predictor of bleeding (HR: 1.7; 95% CI: 1.1-2.5; p < 0.003).
Conclusion: Baseline PNI is an independent predictor of post-discharge bleeding in ACS patients on DAPT after PCI, suggesting it could be a valuable tool for risk stratification of bleeding in these patients.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


