{"title":"Clinical course of children with postinfectious bronchiolitis obliterans with versus without comorbid bronchopulmonary dysplasia.","authors":"Lamia Medghoul, Julien Grosjean, Christophe Marguet, Hortense Petat","doi":"10.3345/cep.2025.00122","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postinfectious bronchiolitis obliterans (PIBO) is a rare chronic obstructive pulmonary disease that occurs after a respiratory infection. Its diagnosis is generally based on clinical history, respiratory symptoms, and computed tomography (CT) findings.</p><p><strong>Purpose: </strong>Here we evaluated the frequency of exacerbations, clinical progress, and inhaled corticosteroid (ICS) usage in children diagnosed with PIBO with or without comorbid bronchopulmonary dysplasia (BPD).</p><p><strong>Methods: </strong>This retrospective observational study was conducted in Rouen, France. The inclusion criteria were as follows: child diagnosed with PIBO (history of respiratory infection, airway obstruction with no or poor response to bronchodilation treatment, and/or mosaic pattern or trapping on chest high-resolution CT) in 2009-2024 treated with intravenous corticosteroid pulses.</p><p><strong>Results: </strong>Fifty-seven patients were included: 13 (23%) with BPD and 44 (77%) without BPD. The mean age at diagnosis was 7.0±3.6 months, with no significant intergroup difference. We observed a significant reduction in exacerbations following corticosteroid pulse treatment as soon as 6 months (P<0.001), with persistent effects observed up to 24 months (P=0.02). We also noted a reduced daily ICS dose starting at 12 months (P=0.03). Respiratory syncytial virus is the most commonly identified causative virus, followed by rhinoviruses and adenoviruses. The viral codetection rates were 18% and 61% in the BPD and non-BPD groups, respectively.</p><p><strong>Conclusion: </strong>In our cohort, intravenous corticosteroid pulse treatment effectively treated PIBO, with a rapid and long-lasting reduction in exacerbations and ICS requirements. BPD was a significant comorbidity of PIBO.</p>","PeriodicalId":36018,"journal":{"name":"Clinical and Experimental Pediatrics","volume":" ","pages":"497-502"},"PeriodicalIF":3.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12235340/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3345/cep.2025.00122","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
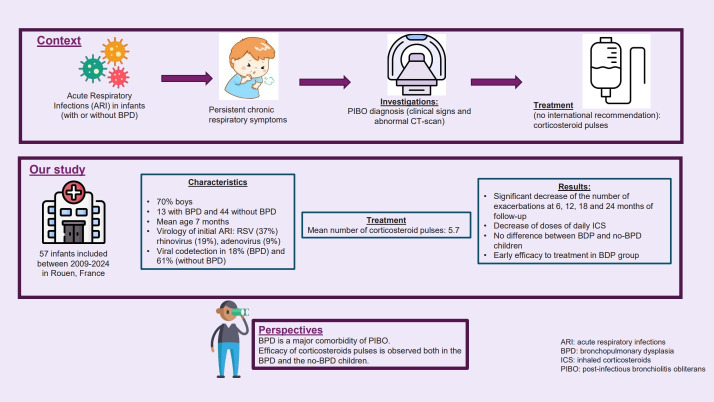
Background: Postinfectious bronchiolitis obliterans (PIBO) is a rare chronic obstructive pulmonary disease that occurs after a respiratory infection. Its diagnosis is generally based on clinical history, respiratory symptoms, and computed tomography (CT) findings.
Purpose: Here we evaluated the frequency of exacerbations, clinical progress, and inhaled corticosteroid (ICS) usage in children diagnosed with PIBO with or without comorbid bronchopulmonary dysplasia (BPD).
Methods: This retrospective observational study was conducted in Rouen, France. The inclusion criteria were as follows: child diagnosed with PIBO (history of respiratory infection, airway obstruction with no or poor response to bronchodilation treatment, and/or mosaic pattern or trapping on chest high-resolution CT) in 2009-2024 treated with intravenous corticosteroid pulses.
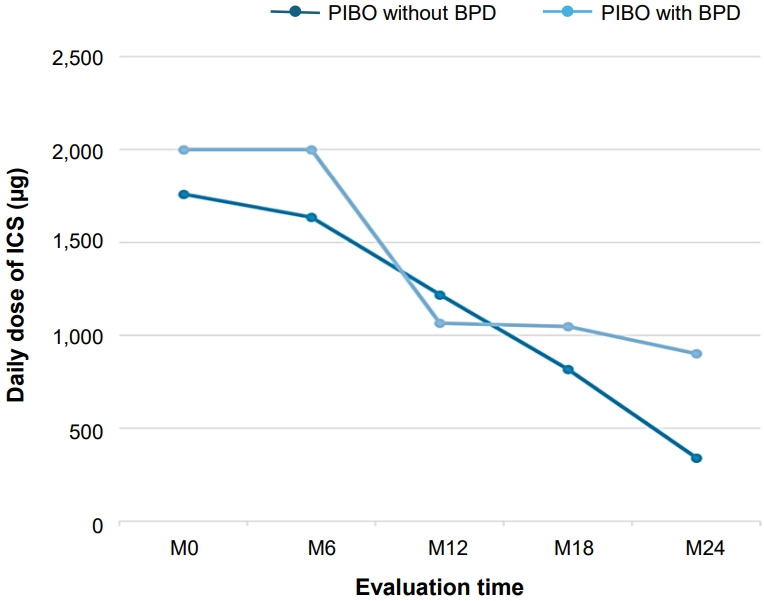
Results: Fifty-seven patients were included: 13 (23%) with BPD and 44 (77%) without BPD. The mean age at diagnosis was 7.0±3.6 months, with no significant intergroup difference. We observed a significant reduction in exacerbations following corticosteroid pulse treatment as soon as 6 months (P<0.001), with persistent effects observed up to 24 months (P=0.02). We also noted a reduced daily ICS dose starting at 12 months (P=0.03). Respiratory syncytial virus is the most commonly identified causative virus, followed by rhinoviruses and adenoviruses. The viral codetection rates were 18% and 61% in the BPD and non-BPD groups, respectively.
Conclusion: In our cohort, intravenous corticosteroid pulse treatment effectively treated PIBO, with a rapid and long-lasting reduction in exacerbations and ICS requirements. BPD was a significant comorbidity of PIBO.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


