Abbreviated 12-Hour Postpartum Magnesium Sulphate Therapy is Equally Effective and Safer Than Standard 24-Hour Therapy in Preeclampsia With Severe Features: Results From A Randomized Controlled Trial.
Pradip Kumar Saha, Seema Sheokand, L K Dhaliwal, Rashmi Bagga, Lekha Saha
{"title":"Abbreviated 12-Hour Postpartum Magnesium Sulphate Therapy is Equally Effective and Safer Than Standard 24-Hour Therapy in Preeclampsia With Severe Features: Results From A Randomized Controlled Trial.","authors":"Pradip Kumar Saha, Seema Sheokand, L K Dhaliwal, Rashmi Bagga, Lekha Saha","doi":"10.18502/jfrh.v19i1.18437","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Eclampsia is a major life-threatening complication of preeclampsia with severe features leading to significant perinatal and maternal mortality and morbidity. Magnesium sulphate (MgSO<sub>4</sub>) is the first-line therapy for eclampsia prevention and treatment, however, its use is associated with serious adverse effects and there is no consensus on the optimal duration of its therapy. This study compares the efficacy and safety of abbreviated 12-hour versus standard 24-hour MgSO<sub>4</sub> therapy during postpartum in patients having preeclampsia with severe features.</p><p><strong>Materials and methods: </strong>Patients having preeclampsia with severe features were randomized 1:1 into the 12-hour and 24-hour groups. Modified Pritchard regimen was used. The primary outcome was the incidence of seizures. Secondary outcomes included serious maternal morbidity and other adverse effects associated with MgSO<sub>4</sub> use. Perinatal outcomes were also recorded. Analyses were intention-to-treat.</p><p><strong>Results: </strong>A total of 116 patients [57 (12-hour group) and 59 (24-hour group)] were included. The mean age was 25(±4) years, while the mean gestation period was 34 (±4) weeks. The incidence of seizures was comparable in the two groups [1 (2%), 3 (5%), p=0.62]. Patients in the 12-hour group [1 (2%)] had lesser postpartum drowsiness compared to the 24-hour group [15 (25%), p<0.001] and consequently, lesser problems in breastfeeding [1 (2%) versus 10 (17%), p=0.008]. There were no inter-group differences in other adverse effects including loss of reflexes, oliguria, respiratory depression, and proportion of patients requiring interruption of therapy. Perinatal outcomes were also similar.</p><p><strong>Conclusion: </strong>In patients having preeclampsia with severe features, 12-hour postpartum MgSO<sub>4</sub> therapy is equally effective in preventing eclampsia and has lesser postpartum drowsiness and problems with breast feeding compared to the standard 24-hour therapy.</p>","PeriodicalId":15845,"journal":{"name":"Journal of Family and Reproductive Health","volume":"19 1","pages":"31-36"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12060206/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Family and Reproductive Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jfrh.v19i1.18437","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Eclampsia is a major life-threatening complication of preeclampsia with severe features leading to significant perinatal and maternal mortality and morbidity. Magnesium sulphate (MgSO4) is the first-line therapy for eclampsia prevention and treatment, however, its use is associated with serious adverse effects and there is no consensus on the optimal duration of its therapy. This study compares the efficacy and safety of abbreviated 12-hour versus standard 24-hour MgSO4 therapy during postpartum in patients having preeclampsia with severe features.
Materials and methods: Patients having preeclampsia with severe features were randomized 1:1 into the 12-hour and 24-hour groups. Modified Pritchard regimen was used. The primary outcome was the incidence of seizures. Secondary outcomes included serious maternal morbidity and other adverse effects associated with MgSO4 use. Perinatal outcomes were also recorded. Analyses were intention-to-treat.
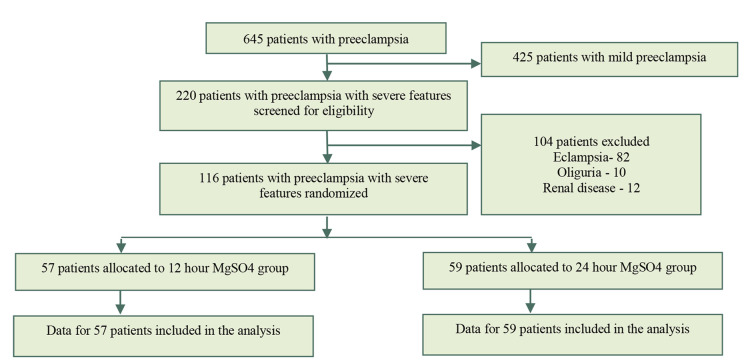
Results: A total of 116 patients [57 (12-hour group) and 59 (24-hour group)] were included. The mean age was 25(±4) years, while the mean gestation period was 34 (±4) weeks. The incidence of seizures was comparable in the two groups [1 (2%), 3 (5%), p=0.62]. Patients in the 12-hour group [1 (2%)] had lesser postpartum drowsiness compared to the 24-hour group [15 (25%), p<0.001] and consequently, lesser problems in breastfeeding [1 (2%) versus 10 (17%), p=0.008]. There were no inter-group differences in other adverse effects including loss of reflexes, oliguria, respiratory depression, and proportion of patients requiring interruption of therapy. Perinatal outcomes were also similar.
Conclusion: In patients having preeclampsia with severe features, 12-hour postpartum MgSO4 therapy is equally effective in preventing eclampsia and has lesser postpartum drowsiness and problems with breast feeding compared to the standard 24-hour therapy.
期刊介绍:
The Journal of Family & Reproductive Health (JFRH) is the quarterly official journal of Vali–e–Asr Reproductive Health Research Center. This journal features fulllength, peerreviewed papers reporting original research, clinical case histories, review articles, as well as opinions and debates on topical issues. Papers published cover the scientific and medical aspects of reproductive physiology and pathology including genetics, endocrinology, andrology, embryology, gynecologic urology, fetomaternal medicine, oncology, infectious disease, public health, nutrition, surgery, menopause, family planning, infertility, psychiatry–psychology, demographic modeling, perinatalogy–neonatolgy ethics and social issues, and pharmacotherapy. A high scientific and editorial standard is maintained throughout the journal along with a regular rate of publication. All published articles will become the property of the JFRH. The editor and publisher accept no responsibility for the statements expressed by the authors here in. Also they do not guarantee, warrant or endorse any product or service advertised in the journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


