Evaluating the Machine Learning Models in Predicting Intensive Care Unit Discharge for Neurosurgical Patients Undergoing Craniotomy: A Big Data Analysis.
Taghi Khaniyev, Efecan Cekic, Muhammet Abdullah Koc, Ilke Dogan, Sahin Hanalioglu
{"title":"Evaluating the Machine Learning Models in Predicting Intensive Care Unit Discharge for Neurosurgical Patients Undergoing Craniotomy: A Big Data Analysis.","authors":"Taghi Khaniyev, Efecan Cekic, Muhammet Abdullah Koc, Ilke Dogan, Sahin Hanalioglu","doi":"10.1007/s12028-025-02246-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Predicting intensive care unit (ICU) discharge for neurosurgical patients is crucial for optimizing bed sources, reducing costs, and improving outcomes. Our study aims to develop and validate machine learning (ML) models to predict ICU discharge within 24 h for patients undergoing craniotomy.</p><p><strong>Methods: </strong>The 2,742 patients undergoing craniotomy were identified from Medical Information Mart for Intensive Care dataset using diagnosis-related group and International Classification of Diseases codes. Demographic, clinical, laboratory, and radiological data were collected and preprocessed. Textual clinical examinations were converted into numerical scales. Data were split into training (70%), validation (15%), and test (15%) sets. Four ML models, logistic regression (LR), decision tree, random forest, and neural network (NN), were trained and evaluated. Model performance was assessed using area under the receiver operating characteristic curve (AUC), average precision (AP), accuracy, and F1 scores. Shapley Additive Explanations (SHAP) were used to analyze importance of features. Statistical analyses were performed using R (version 4.2.1) and ML analyses with Python (version 3.8), using scikit-learn, tensorflow, and shap packages.</p><p><strong>Results: </strong>Cohort included 2,742 patients (mean age 58.2 years; first and third quartiles 47-70 years), with 53.4% being male (n = 1,464). Total ICU stay was 15,645 bed days (mean length of stay 4.7 days), and total hospital stay was 32,008 bed days (mean length of stay 10.8 days). Random forest demonstrated highest performance (AUC 0.831, AP 0.561, accuracy 0.827, F1-score 0.339) on test set. NN achieved an AUC of 0.824, with an AP, accuracy, and F1-score of 0.558, 0.830, and 0.383, respectively. LR achieved an AUC of 0.821 and an accuracy of 0.829. The decision tree model showed lowest performance (AUC 0.813, accuracy 0.822). Key predictors of SHAP analysis included Glasgow Coma Scale, respiratory-related parameters (i.e., tidal volume, respiratory effort), intracranial pressure, arterial pH, and Richmond Agitation-Sedation Scale.</p><p><strong>Conclusions: </strong>Random forest and NN predict ICU discharge well, whereas LR is interpretable but less accurate. Numeric conversion of clinical data improved performance. This study offers framework for predictions using clinical, radiological, and demographic features, with SHAP enhancing transparency.</p>","PeriodicalId":19118,"journal":{"name":"Neurocritical Care","volume":" ","pages":"512-529"},"PeriodicalIF":3.6000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436523/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurocritical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12028-025-02246-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Predicting intensive care unit (ICU) discharge for neurosurgical patients is crucial for optimizing bed sources, reducing costs, and improving outcomes. Our study aims to develop and validate machine learning (ML) models to predict ICU discharge within 24 h for patients undergoing craniotomy.
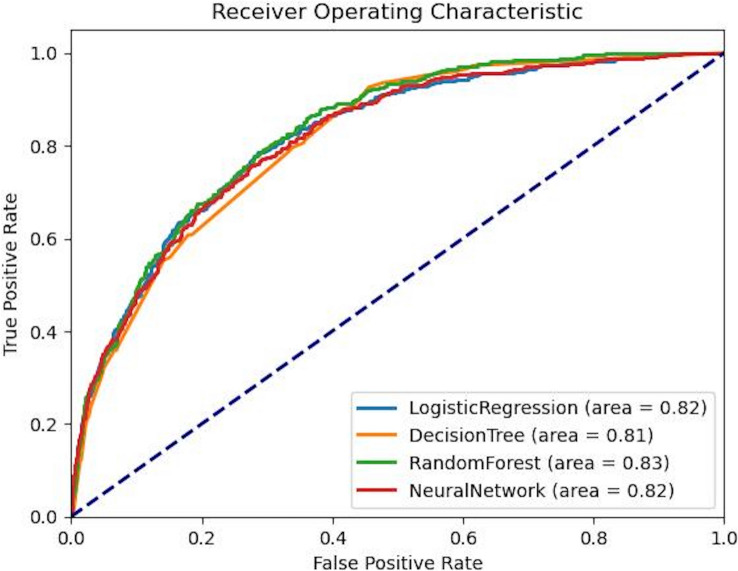
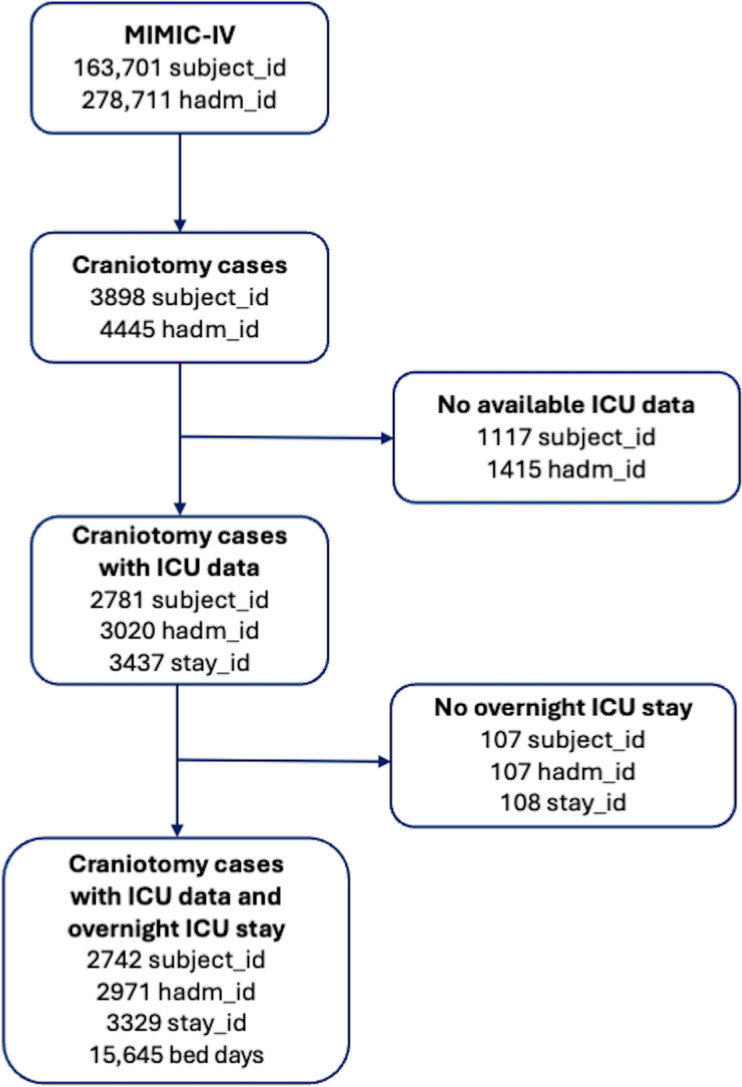
Methods: The 2,742 patients undergoing craniotomy were identified from Medical Information Mart for Intensive Care dataset using diagnosis-related group and International Classification of Diseases codes. Demographic, clinical, laboratory, and radiological data were collected and preprocessed. Textual clinical examinations were converted into numerical scales. Data were split into training (70%), validation (15%), and test (15%) sets. Four ML models, logistic regression (LR), decision tree, random forest, and neural network (NN), were trained and evaluated. Model performance was assessed using area under the receiver operating characteristic curve (AUC), average precision (AP), accuracy, and F1 scores. Shapley Additive Explanations (SHAP) were used to analyze importance of features. Statistical analyses were performed using R (version 4.2.1) and ML analyses with Python (version 3.8), using scikit-learn, tensorflow, and shap packages.
Results: Cohort included 2,742 patients (mean age 58.2 years; first and third quartiles 47-70 years), with 53.4% being male (n = 1,464). Total ICU stay was 15,645 bed days (mean length of stay 4.7 days), and total hospital stay was 32,008 bed days (mean length of stay 10.8 days). Random forest demonstrated highest performance (AUC 0.831, AP 0.561, accuracy 0.827, F1-score 0.339) on test set. NN achieved an AUC of 0.824, with an AP, accuracy, and F1-score of 0.558, 0.830, and 0.383, respectively. LR achieved an AUC of 0.821 and an accuracy of 0.829. The decision tree model showed lowest performance (AUC 0.813, accuracy 0.822). Key predictors of SHAP analysis included Glasgow Coma Scale, respiratory-related parameters (i.e., tidal volume, respiratory effort), intracranial pressure, arterial pH, and Richmond Agitation-Sedation Scale.
Conclusions: Random forest and NN predict ICU discharge well, whereas LR is interpretable but less accurate. Numeric conversion of clinical data improved performance. This study offers framework for predictions using clinical, radiological, and demographic features, with SHAP enhancing transparency.
期刊介绍:
Neurocritical Care is a peer reviewed scientific publication whose major goal is to disseminate new knowledge on all aspects of acute neurological care. It is directed towards neurosurgeons, neuro-intensivists, neurologists, anesthesiologists, emergency physicians, and critical care nurses treating patients with urgent neurologic disorders. These are conditions that may potentially evolve rapidly and could need immediate medical or surgical intervention. Neurocritical Care provides a comprehensive overview of current developments in intensive care neurology, neurosurgery and neuroanesthesia and includes information about new therapeutic avenues and technological innovations. Neurocritical Care is the official journal of the Neurocritical Care Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


