Defining advanced lymph node metastasis in intrahepatic cholangiocarcinoma: A multicenter study
Abstract
Background
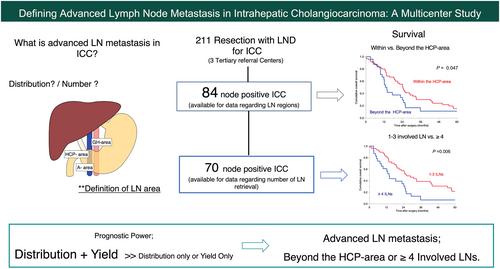
There is no specific boundary for stratifying survival outcomes in patients with node-positive intrahepatic cholangiocarcinoma (ICC). This study aimed to propose advanced nodal status in ICC.
Methods
Data from patients with pathologically confirmed node-positive ICC who underwent liver resection (LR) with lymph node dissection (LND) from 2000 to 2020 at three tertiary centers were retrospectively analyzed. The boundaries of regions and the yield that stratified overall survival (OS) were evaluated. The lymph node (LN) regions were defined as follows: hepatoduodenal ligament, common hepatic artery, and peripancreatic area (HCP-area), gastrohepatic area (GH-area), and para-aortic area (A-area).
Results
Eighty-four patients with node-positive ICC were enrolled in this study. The median numbers of retrieved LNs and involved LNs (ILNs) were 15 (range: 2–56) and 2 (range: 1–20), respectively. Most patients (96.5%) had ILNs in the HCP-area, whereas only 3 patients (3.5%) had ILNs in other areas without HCP-area involvement. OS of patients with LN metastasis confined to the HCP-area was better than for those beyond this area (median OS: 24.3 vs. 13.3 months, p = 0.047). The best cut-off number of ILNs to stratify OS was 4, and patients with 1–3 ILNs showed better OS than those with ≥ 4 ILNs (25.4 vs. 13.8 months, p = 0.006). Combining distribution and yield showed the best prognostic power compared to using either distribution or yield alone.
Conclusion
In patients with node-positive ICC, LN metastasis beyond the HCP-area or ≥ 4 ILNs can be proposed as advanced N disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


