{"title":"MOG positive primary autoimmune meningitis mimicking tuberculous meningitis: a case series.","authors":"Tejas Shivarthi, Mahima Sriram, Muddana Nikhilesh, Sudheeran Kannoth, Vivek Nambiar, Siby Gopinath, Saraf Udit Umesh, Gopikrishnan Unnikrishnan, Anand Kumar, Annamma Mathai, Meena Thevarkalam","doi":"10.1136/bmjno-2024-000999","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Primary autoimmune meningitis presentation of myelin oligodendrocyte glycoprotein (MOG) IgG antibody positivity is infrequently reported. We aim to identify the patients with MOG IgG antibody positivity who were initially misdiagnosed and treated as tuberculous meningitis (TBM).</p><p><strong>Methods: </strong>A retrospective cross-sectional study conducted in the Neuroimmunology Laboratory and Department of Neurology of Amrita Institute of Medical Sciences, Kochi, Kerala, India between June 2018 and December 2023. MOG IgG antibody positive cases were identified from the Neuroimmunology Lab Registry, and the case sheets were screened for TBM-like presentation. Cases were included on the basis of MOG IgG positivity, an initial diagnosis of tuberculosis was suspected and antitubercular therapy was initiated with minimal response.</p><p><strong>Results: </strong>We described the clinical, microbiological, radiological and serological features of five patients with a TBM-like presentation eventually diagnosed with MOG-associated meningitis. Symptoms included headache, vomiting, visual impairment and weakness. Three patients showed normal MRIs and two patients showed MRI findings consistent with demyelination. Serum MOG antibody testing was positive only on serial testing of all five patients. The final diagnosis was MOG-associated meningitis in two patients and MOG-associated meningoencephalitis in three patients.</p><p><strong>Discussion: </strong>This case series highlights the rare presentation of MOG antibody positive patients presenting as primary autoimmune meningitis and its diagnostic challenges, especially in regions where tuberculosis is common. The study underscores the importance of considering autoimmune aetiology as a differential diagnosis when tuberculosis treatment fails or relapses occur, advocating for MOG IgG antibody testing to ensure accurate diagnosis and effective treatment.</p>","PeriodicalId":52754,"journal":{"name":"BMJ Neurology Open","volume":"7 1","pages":"e000999"},"PeriodicalIF":2.4000,"publicationDate":"2025-04-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12035451/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Neurology Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjno-2024-000999","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Primary autoimmune meningitis presentation of myelin oligodendrocyte glycoprotein (MOG) IgG antibody positivity is infrequently reported. We aim to identify the patients with MOG IgG antibody positivity who were initially misdiagnosed and treated as tuberculous meningitis (TBM).
Methods: A retrospective cross-sectional study conducted in the Neuroimmunology Laboratory and Department of Neurology of Amrita Institute of Medical Sciences, Kochi, Kerala, India between June 2018 and December 2023. MOG IgG antibody positive cases were identified from the Neuroimmunology Lab Registry, and the case sheets were screened for TBM-like presentation. Cases were included on the basis of MOG IgG positivity, an initial diagnosis of tuberculosis was suspected and antitubercular therapy was initiated with minimal response.
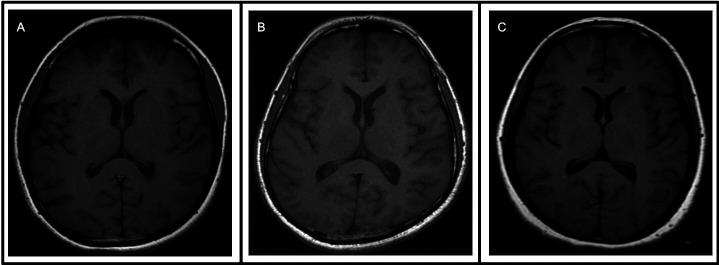
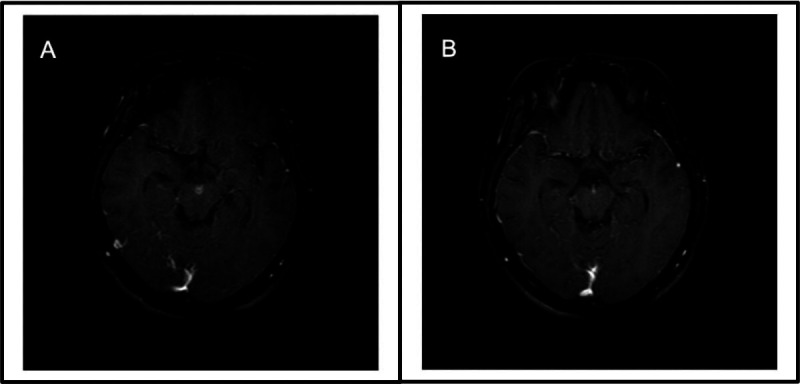
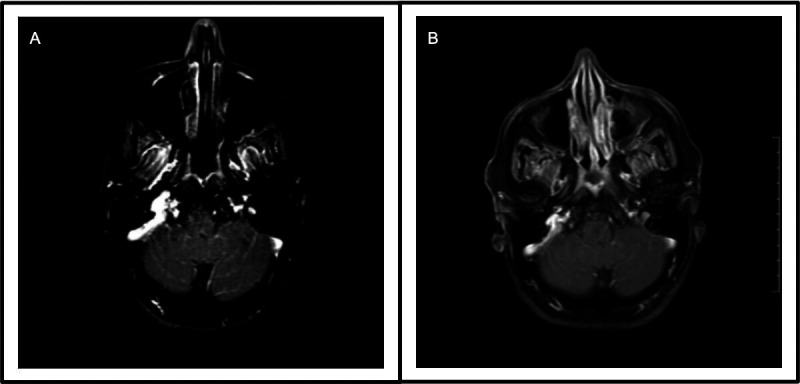
Results: We described the clinical, microbiological, radiological and serological features of five patients with a TBM-like presentation eventually diagnosed with MOG-associated meningitis. Symptoms included headache, vomiting, visual impairment and weakness. Three patients showed normal MRIs and two patients showed MRI findings consistent with demyelination. Serum MOG antibody testing was positive only on serial testing of all five patients. The final diagnosis was MOG-associated meningitis in two patients and MOG-associated meningoencephalitis in three patients.
Discussion: This case series highlights the rare presentation of MOG antibody positive patients presenting as primary autoimmune meningitis and its diagnostic challenges, especially in regions where tuberculosis is common. The study underscores the importance of considering autoimmune aetiology as a differential diagnosis when tuberculosis treatment fails or relapses occur, advocating for MOG IgG antibody testing to ensure accurate diagnosis and effective treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


