{"title":"Optimizing Diabetic Retinopathy Screening at Primary Health Centres in India: A Cost-Effectiveness Analysis.","authors":"Neha Purohit, Parul Chawla Gupta, Sandeep Buttan, Akashdeep Singh Chauhan, Ranjan Kumar Choudhury, Vishali Gupta, Atul Kotwal, Shankar Prinja","doi":"10.1007/s41669-025-00572-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The eye care package under the Ayushman Bharat comprehensive primary healthcare programme includes annual population-based screening for diabetic retinopathy (DR) using non-mydriatic fundus cameras at the primary health centres (PHCs) in India. However, there can be several implementation models for introduction of a systematic screening programme for DR.</p><p><strong>Objectives: </strong>This study aims to assess the cost effectiveness of screening for DR in comparison with the usual-care scenario without a DR screening programme, and to determine cost-effective approaches for implementation of annual population-based screening for DR by optometrists at PHCs in India in terms of screening modalities (face-to-face vs tele-supported screening [screening followed by transfer and remote grading of images by ophthalmologists] vs artificial intelligence [AI]-supported screening) and target population groups for screening.</p><p><strong>Methods: </strong>A mathematical model comprising a decision tree and Markov model was developed. An extensive review of published literature was undertaken to obtain model parameters. Primary data collection was done to derive quality-of-life values. We used a lifetime horizon, abridged societal perspective, and discounted future costs and consequences at an annual rate of 3%. The incremental cost-effectiveness ratio (ICER) was computed for alternative screening strategies. A willingness-to-pay equal to gross domestic product per capita equal to ₹171,498 (US$2182) was used to determine the cost-effective choice. Sensitivity analyses were performed to assess the impact of variation in input parameters on the ICER values.</p><p><strong>Results: </strong>All the annual screening strategies were found to have lower ICERs relative to usual care. Among the screening strategies, annual tele-supported screening in the population with diabetes duration ≥5 years was the most cost-effective strategy with an ICER value of ₹57,408 (US$730) per quality-adjusted life year (QALY) gained. At the national level, this strategy is likely to reduce the annual incidence of vision-threatening DR and blindness by 17.3%, and 38.5%, respectively, and would result in higher benefits in Indian states with higher epidemiological transition. Sensitivity analyses showed that if adequate glycaemic control is achieved in 79% of the diabetic population, annual AI-supported screening in individuals with a diabetes' duration of 10 years or more becomes the most cost-effective strategy.</p><p><strong>Conclusion: </strong>The results of the study suggest the prioritization of an annual tele-supported DR screening programme in India. They also highlight the importance of the adoption of an integrated approach and functional linkage between eye care and diabetes care, to intensify efforts directed at improving glycaemic control, and to facilitate early DR detection and management.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"627-638"},"PeriodicalIF":2.1000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12209073/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-025-00572-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The eye care package under the Ayushman Bharat comprehensive primary healthcare programme includes annual population-based screening for diabetic retinopathy (DR) using non-mydriatic fundus cameras at the primary health centres (PHCs) in India. However, there can be several implementation models for introduction of a systematic screening programme for DR.
Objectives: This study aims to assess the cost effectiveness of screening for DR in comparison with the usual-care scenario without a DR screening programme, and to determine cost-effective approaches for implementation of annual population-based screening for DR by optometrists at PHCs in India in terms of screening modalities (face-to-face vs tele-supported screening [screening followed by transfer and remote grading of images by ophthalmologists] vs artificial intelligence [AI]-supported screening) and target population groups for screening.
Methods: A mathematical model comprising a decision tree and Markov model was developed. An extensive review of published literature was undertaken to obtain model parameters. Primary data collection was done to derive quality-of-life values. We used a lifetime horizon, abridged societal perspective, and discounted future costs and consequences at an annual rate of 3%. The incremental cost-effectiveness ratio (ICER) was computed for alternative screening strategies. A willingness-to-pay equal to gross domestic product per capita equal to ₹171,498 (US$2182) was used to determine the cost-effective choice. Sensitivity analyses were performed to assess the impact of variation in input parameters on the ICER values.
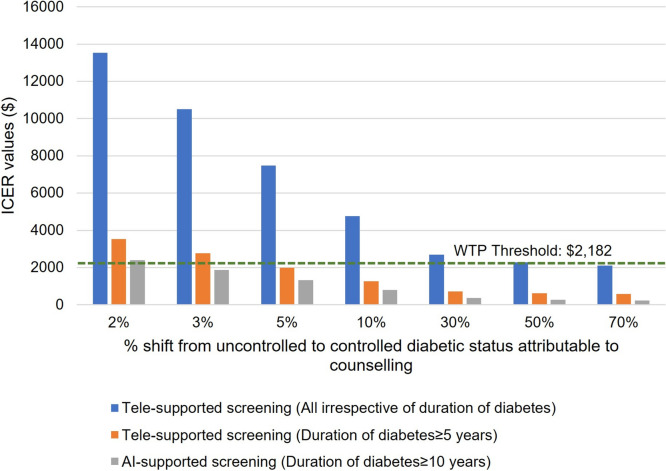
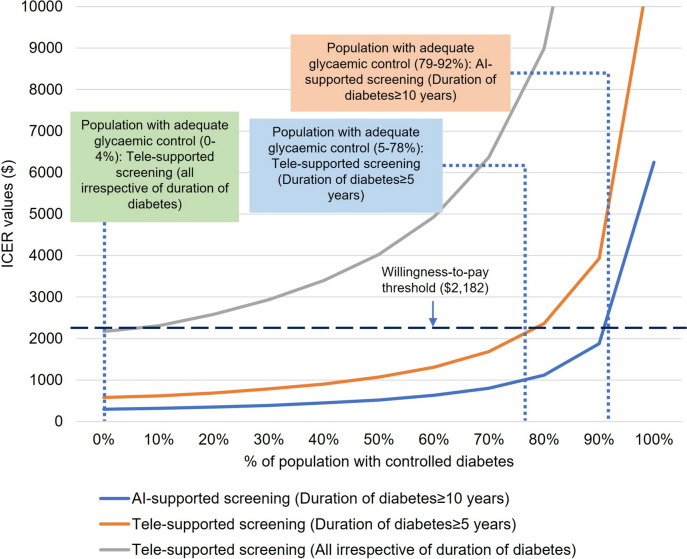
Results: All the annual screening strategies were found to have lower ICERs relative to usual care. Among the screening strategies, annual tele-supported screening in the population with diabetes duration ≥5 years was the most cost-effective strategy with an ICER value of ₹57,408 (US$730) per quality-adjusted life year (QALY) gained. At the national level, this strategy is likely to reduce the annual incidence of vision-threatening DR and blindness by 17.3%, and 38.5%, respectively, and would result in higher benefits in Indian states with higher epidemiological transition. Sensitivity analyses showed that if adequate glycaemic control is achieved in 79% of the diabetic population, annual AI-supported screening in individuals with a diabetes' duration of 10 years or more becomes the most cost-effective strategy.
Conclusion: The results of the study suggest the prioritization of an annual tele-supported DR screening programme in India. They also highlight the importance of the adoption of an integrated approach and functional linkage between eye care and diabetes care, to intensify efforts directed at improving glycaemic control, and to facilitate early DR detection and management.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


