David Beckmann, Moritz Flick, Karim Kouz, Bernd Saugel
{"title":"A smartphone application for semi-automated QT interval analysis based on a snapshot of an electrocardiogram trace displayed on a patient monitor.","authors":"David Beckmann, Moritz Flick, Karim Kouz, Bernd Saugel","doi":"10.1007/s10877-025-01277-z","DOIUrl":null,"url":null,"abstract":"<p><p>We developed a smartphone application (SMART-QT application) that can semi-automatically measure QT and QTc intervals based on a snapshot of the electrocardiogram (ECG) trace and the heart rate displayed on a patient monitor. In this study, we aimed to validate the SMART-QT application. In this prospective single-center method comparison study, we measured QT and QTc intervals with the SMART-QT application (QT<sub>APP</sub> and QTc<sub>APP</sub>; test method) and simultaneously manually measured QT and QTc intervals from a 12-lead ECG (QT<sub>REF</sub> and QTc<sub>REF</sub>; reference method) in 57 adult volunteers and patients who had sinus rhythm and no acute or chronic cardiac comorbidities. To investigate the agreement between QT<sub>APP</sub> and QT<sub>REF</sub> and between QTc<sub>APP</sub> and QTc<sub>REF</sub>, we performed Bland-Altman analyses and calculated the mean of the differences, the standard deviation, and the 95%-limits of agreement (95%-LOA). We defined clinically acceptable agreement as maximum mean of the differences ± standard deviation of 20 ± 20 ms. The mean of the differences between QT<sub>APP</sub> and QT<sub>REF</sub> was 14 ± 20 ms (95%-LOA -26 to 54 ms). The mean of the differences between QTc<sub>APP</sub> and QTc<sub>REF</sub> was 13 ± 15 ms (95%-LOA -16 to 42 ms). The agreement between QT<sub>APP</sub> and QT<sub>REF</sub> and between QTc<sub>APP</sub> and QTc<sub>REF</sub> was clinically acceptable in adult volunteers and patients without cardiac comorbidities.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"787-791"},"PeriodicalIF":2.2000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304064/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-025-01277-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
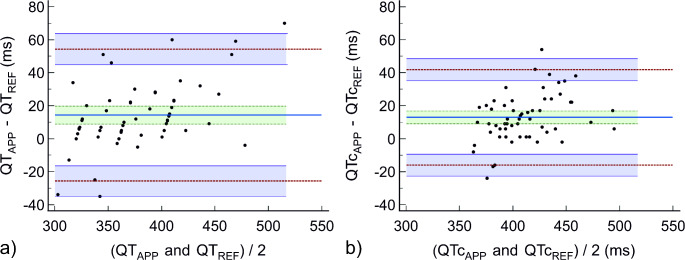
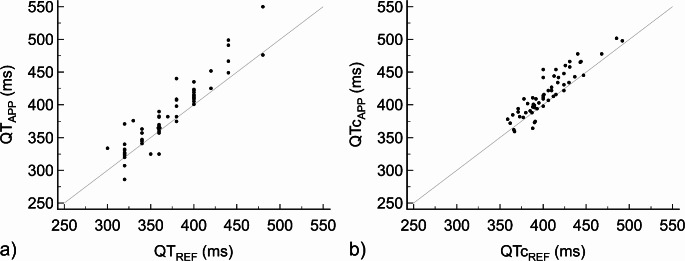
We developed a smartphone application (SMART-QT application) that can semi-automatically measure QT and QTc intervals based on a snapshot of the electrocardiogram (ECG) trace and the heart rate displayed on a patient monitor. In this study, we aimed to validate the SMART-QT application. In this prospective single-center method comparison study, we measured QT and QTc intervals with the SMART-QT application (QTAPP and QTcAPP; test method) and simultaneously manually measured QT and QTc intervals from a 12-lead ECG (QTREF and QTcREF; reference method) in 57 adult volunteers and patients who had sinus rhythm and no acute or chronic cardiac comorbidities. To investigate the agreement between QTAPP and QTREF and between QTcAPP and QTcREF, we performed Bland-Altman analyses and calculated the mean of the differences, the standard deviation, and the 95%-limits of agreement (95%-LOA). We defined clinically acceptable agreement as maximum mean of the differences ± standard deviation of 20 ± 20 ms. The mean of the differences between QTAPP and QTREF was 14 ± 20 ms (95%-LOA -26 to 54 ms). The mean of the differences between QTcAPP and QTcREF was 13 ± 15 ms (95%-LOA -16 to 42 ms). The agreement between QTAPP and QTREF and between QTcAPP and QTcREF was clinically acceptable in adult volunteers and patients without cardiac comorbidities.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


