Kenyon W Osborne, Wiremu S MacFater, Brian J Anderson, Darren Svirskis, Andrew G Hill, Jacqueline A Hannam
{"title":"Pharmacokinetics of Intraperitoneal Lidocaine for Sustained Postoperative Analgesia in Adults.","authors":"Kenyon W Osborne, Wiremu S MacFater, Brian J Anderson, Darren Svirskis, Andrew G Hill, Jacqueline A Hannam","doi":"10.1007/s13318-025-00948-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Intraperitoneal lidocaine is an emerging strategy for analgesia following abdominal surgery but its pharmacokinetics are poorly quantified. We aimed to develop a pharmacokinetic model for unbound and total lidocaine by intraperitoneal and intravenous routes.</p><p><strong>Methods: </strong>Unbound and total lidocaine concentrations, and pain scores (visual analogue score 0-10) were from a published randomized control trial of adults (n = 56) undergoing laparoscopic colon resection. Participants received intravenous or intraperitoneal lidocaine (2 mg/kg bolus then 1.5 mg/kg/h infusion) for 72 h postoperatively. Data were pooled with literature-derived alpha-1-acid glycoprotein concentrations (AAG) to support total lidocaine modelling. Unbound kinetics were described using compartmental models with first order absorption between intraperitoneal and plasma compartments. A turnover model described AAG kinetics with constant binding to lidocaine. An inhibitory pharmacodynamic model was explored to link concentration to pain scores.</p><p><strong>Results: </strong>Maximum lidocaine concentrations after intraperitoneal administration were means (range) of 3.0 (0.4-4.5) mg/L total and 0.6 (0.1-0.9) mg/L unbound. Intraperitoneal absorption was incomplete (bioavailability = 0.66, 95% confidence interval (CI) 0.6-0.76) with a half-time of 0.5 (0.4-0.8) h. A two-compartment model with first order elimination fit best, with unbound clearance 121 (108-136) L/h/70 kg. The binding constant to AAG (K<sub>D</sub>) was 2.98 (2.69-3.35) µmol/L. A pharmacodynamic model with C<sub>50</sub> of 0.21 mg/L and maximal reduction (E<sub>max</sub>) of 6 units captured pain scores and was used to simulate dosing strategies.</p><p><strong>Conclusions: </strong>A third of the intraperitoneal dose did not reach the central compartment and absorption took ~2 h. Simulations show that 2 mg/kg/h intraperitoneal infusion achieves a 5-point pain score reduction within ~36 min.</p>","PeriodicalId":11939,"journal":{"name":"European Journal of Drug Metabolism and Pharmacokinetics","volume":" ","pages":"295-306"},"PeriodicalIF":2.4000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227458/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Drug Metabolism and Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s13318-025-00948-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/8 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: Intraperitoneal lidocaine is an emerging strategy for analgesia following abdominal surgery but its pharmacokinetics are poorly quantified. We aimed to develop a pharmacokinetic model for unbound and total lidocaine by intraperitoneal and intravenous routes.
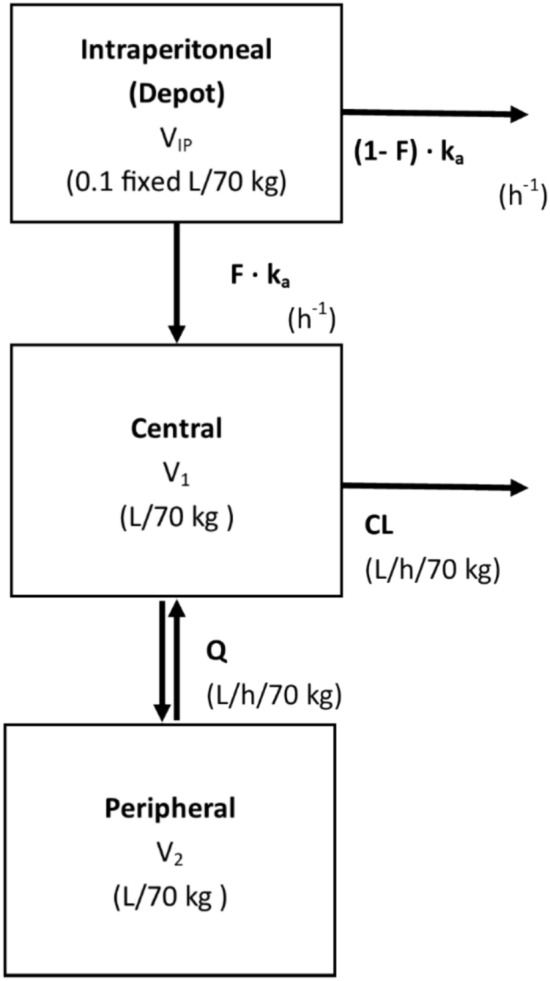
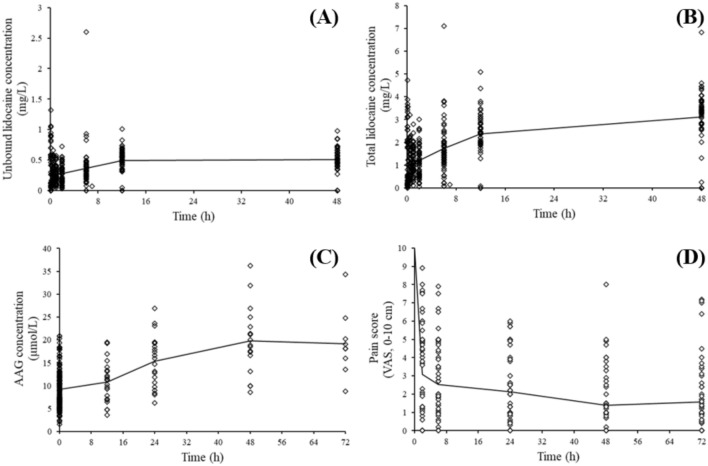
Methods: Unbound and total lidocaine concentrations, and pain scores (visual analogue score 0-10) were from a published randomized control trial of adults (n = 56) undergoing laparoscopic colon resection. Participants received intravenous or intraperitoneal lidocaine (2 mg/kg bolus then 1.5 mg/kg/h infusion) for 72 h postoperatively. Data were pooled with literature-derived alpha-1-acid glycoprotein concentrations (AAG) to support total lidocaine modelling. Unbound kinetics were described using compartmental models with first order absorption between intraperitoneal and plasma compartments. A turnover model described AAG kinetics with constant binding to lidocaine. An inhibitory pharmacodynamic model was explored to link concentration to pain scores.
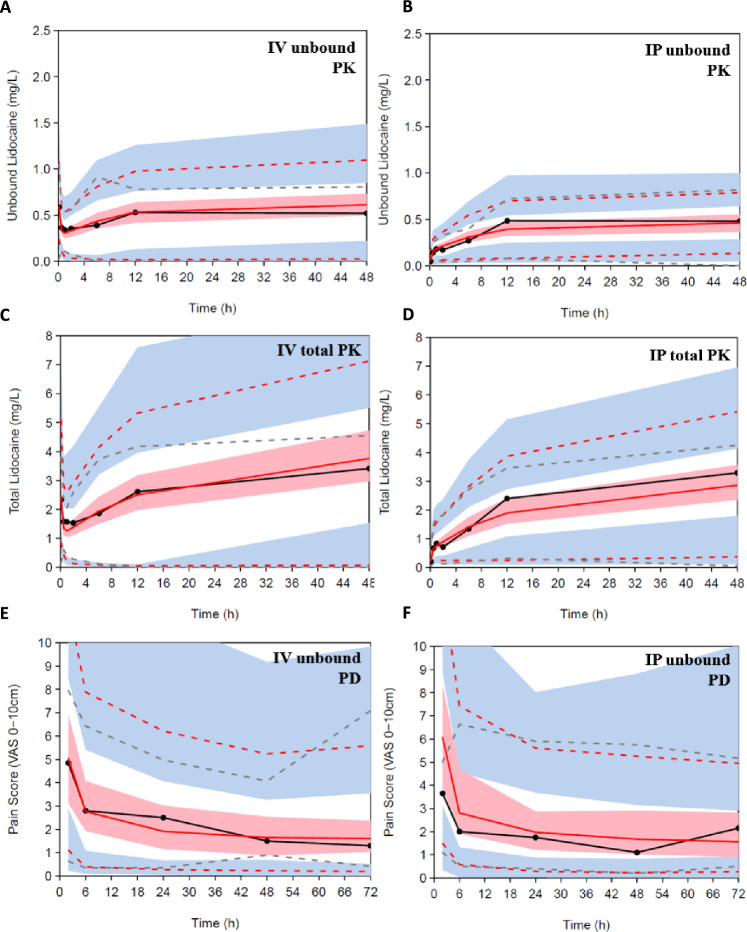
Results: Maximum lidocaine concentrations after intraperitoneal administration were means (range) of 3.0 (0.4-4.5) mg/L total and 0.6 (0.1-0.9) mg/L unbound. Intraperitoneal absorption was incomplete (bioavailability = 0.66, 95% confidence interval (CI) 0.6-0.76) with a half-time of 0.5 (0.4-0.8) h. A two-compartment model with first order elimination fit best, with unbound clearance 121 (108-136) L/h/70 kg. The binding constant to AAG (KD) was 2.98 (2.69-3.35) µmol/L. A pharmacodynamic model with C50 of 0.21 mg/L and maximal reduction (Emax) of 6 units captured pain scores and was used to simulate dosing strategies.
Conclusions: A third of the intraperitoneal dose did not reach the central compartment and absorption took ~2 h. Simulations show that 2 mg/kg/h intraperitoneal infusion achieves a 5-point pain score reduction within ~36 min.
期刊介绍:
Hepatology International is a peer-reviewed journal featuring articles written by clinicians, clinical researchers and basic scientists is dedicated to research and patient care issues in hepatology. This journal focuses mainly on new and emerging diagnostic and treatment options, protocols and molecular and cellular basis of disease pathogenesis, new technologies, in liver and biliary sciences.
Hepatology International publishes original research articles related to clinical care and basic research; review articles; consensus guidelines for diagnosis and treatment; invited editorials, and controversies in contemporary issues. The journal does not publish case reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


