{"title":"Evaluation of a score for identifying hospital stays that trigger a pharmacist intervention: integration into a clinical decision support system.","authors":"Laurine Robert, Nathalie Vidoni, Erwin Gérard, Emmanuel Chazard, Pascal Odou, Chloé Rousselière, Bertrand Décaudin","doi":"10.1093/jamiaopen/ooaf030","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The objective of the study was to determine, after medication review, the patient risk score threshold that would distinguish between stays with prescriptions triggering pharmacist intervention (PI) and stays with prescriptions not triggering PI.</p><p><strong>Materials and methods: </strong>The study was retrospective and observational, conducted in the clinical pharmacy team. The patient risk score was adapted from a Canadian score and was integrated in the clinical decision support system (CDSS). For each hospital stay, the score was calculated at the beginning of hospitalization and we retrospectively showed if a medication review and a PI were conducted. Then, the optimal patient risk score threshold was determined to help pharmacist in optimizing medication review.</p><p><strong>Results: </strong>During the study, 973 (56.7%) medication reviews were performed and 248 (25.5%) led to a PI. After analyzing sensitivity, specificity, and positive predictive value of different thresholds, the threshold of 4 was deemed discriminating to identify hospital stays likely to lead to a PI following a medication review. At this threshold, 600 hospital stays would have been detected (33.3% of the latter led to a PI), and 5.0% of stays with a medication review would not have been detected even though they were hospital stays that had triggered a PI.</p><p><strong>Discussion and conclusion: </strong>Integration of a patient risk score in a CDSS can help clinical pharmacist to target hospital stays likely to trigger a PI. However, an optimal threshold is difficult to determine. Constructing and using a score in practice should be organized with the local clinical pharmacy team, in order to understand the tool's limitations and maximize its use in detecting at-risk drug prescriptions.</p>","PeriodicalId":36278,"journal":{"name":"JAMIA Open","volume":"8 3","pages":"ooaf030"},"PeriodicalIF":3.4000,"publicationDate":"2025-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12051848/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMIA Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jamiaopen/ooaf030","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The objective of the study was to determine, after medication review, the patient risk score threshold that would distinguish between stays with prescriptions triggering pharmacist intervention (PI) and stays with prescriptions not triggering PI.
Materials and methods: The study was retrospective and observational, conducted in the clinical pharmacy team. The patient risk score was adapted from a Canadian score and was integrated in the clinical decision support system (CDSS). For each hospital stay, the score was calculated at the beginning of hospitalization and we retrospectively showed if a medication review and a PI were conducted. Then, the optimal patient risk score threshold was determined to help pharmacist in optimizing medication review.
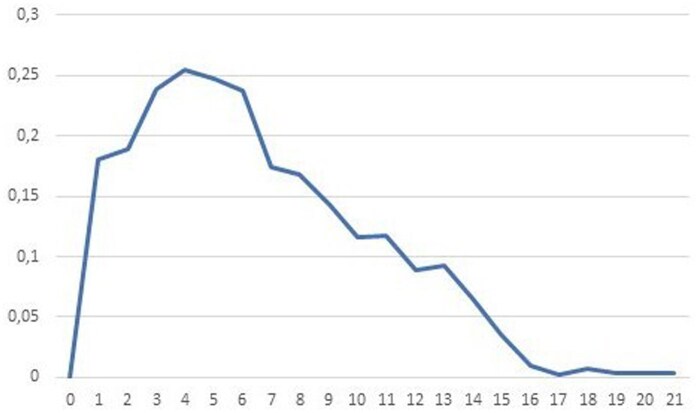
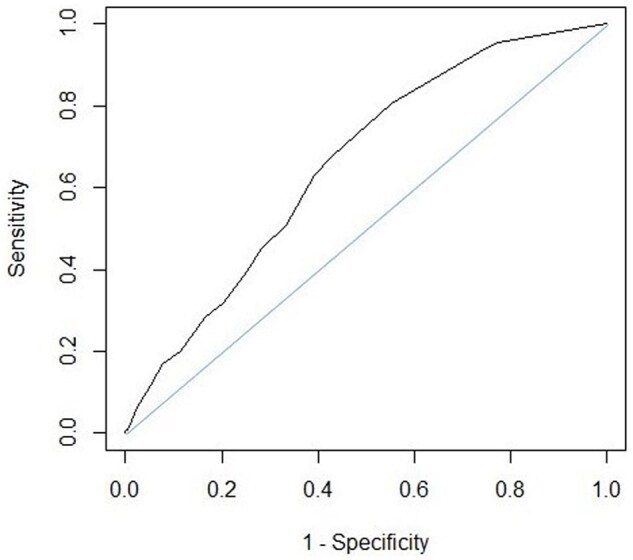
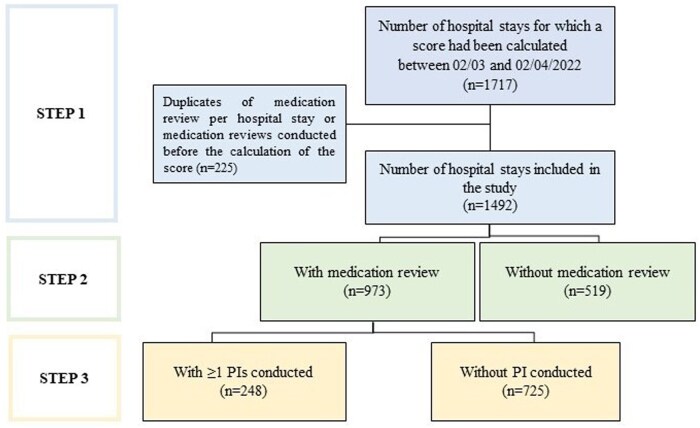
Results: During the study, 973 (56.7%) medication reviews were performed and 248 (25.5%) led to a PI. After analyzing sensitivity, specificity, and positive predictive value of different thresholds, the threshold of 4 was deemed discriminating to identify hospital stays likely to lead to a PI following a medication review. At this threshold, 600 hospital stays would have been detected (33.3% of the latter led to a PI), and 5.0% of stays with a medication review would not have been detected even though they were hospital stays that had triggered a PI.
Discussion and conclusion: Integration of a patient risk score in a CDSS can help clinical pharmacist to target hospital stays likely to trigger a PI. However, an optimal threshold is difficult to determine. Constructing and using a score in practice should be organized with the local clinical pharmacy team, in order to understand the tool's limitations and maximize its use in detecting at-risk drug prescriptions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


