From treatment to threat: the fatal impact of cumulative glucocorticoid dosage on outcomes in immunocompromised patients with community-acquired pneumonia.
{"title":"From treatment to threat: the fatal impact of cumulative glucocorticoid dosage on outcomes in immunocompromised patients with community-acquired pneumonia.","authors":"Saibin Wang, Qian Ye, Yijun Sheng","doi":"10.1177/17534666251332085","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic glucocorticoid therapy is known to heighten the risk of secondary pulmonary infections. However, the impact of cumulative glucocorticoid dosage (CGD) on mortality risk in patients who develop community-acquired pneumonia (CAP) while undergoing glucocorticoid therapy remains inadequately explored.</p><p><strong>Objectives: </strong>This study aims to clarify the relationship between CGD and mortality outcomes in immunocompromised patients with CAP.</p><p><strong>Design: </strong>This study is a retrospective cohort analysis utilizing data from the DRYAD database.</p><p><strong>Methods: </strong>We examined data from 561 patients diagnosed with CAP who had received either oral or intravenous glucocorticoids prior to their CAP diagnosis. To evaluate the effect of CGD on mortality risk, we employed piecewise linear regression and Cox regression analyses, adjusting for relevant confounders.</p><p><strong>Results: </strong>Among the study population, the median CGD was 4 g of methylprednisolone (interquartile range 2.16-8.80 g). The 30-, 60-, and 90-day mortality rates were 22.28%, 25.13%, and 25.49%, respectively. Piecewise linear regression analysis revealed a nonlinear relationship between methylprednisolone dose and mortality risk, indicating a threshold effect at a methylprednisolone level of 20 g. In addition, Cox regression analysis showed a significantly higher mortality risk in patients with CGD exceeding 40 g of methylprednisolone compared to those with CGD between 20 and 40 g, after adjusting for potential confounding factors (adjusted HR 5.16, 95% CI: 1.16-22.99, <i>p</i> < 0.05).</p><p><strong>Conclusion: </strong>CAP occurring in close proximity to recent high doses of steroids is associated with pathogens typically seen in immunocompromised hosts and is linked to higher mortality compared to usual CAP.</p>","PeriodicalId":22884,"journal":{"name":"Therapeutic Advances in Respiratory Disease","volume":"19 ","pages":"17534666251332085"},"PeriodicalIF":3.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12033499/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17534666251332085","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Chronic glucocorticoid therapy is known to heighten the risk of secondary pulmonary infections. However, the impact of cumulative glucocorticoid dosage (CGD) on mortality risk in patients who develop community-acquired pneumonia (CAP) while undergoing glucocorticoid therapy remains inadequately explored.
Objectives: This study aims to clarify the relationship between CGD and mortality outcomes in immunocompromised patients with CAP.
Design: This study is a retrospective cohort analysis utilizing data from the DRYAD database.
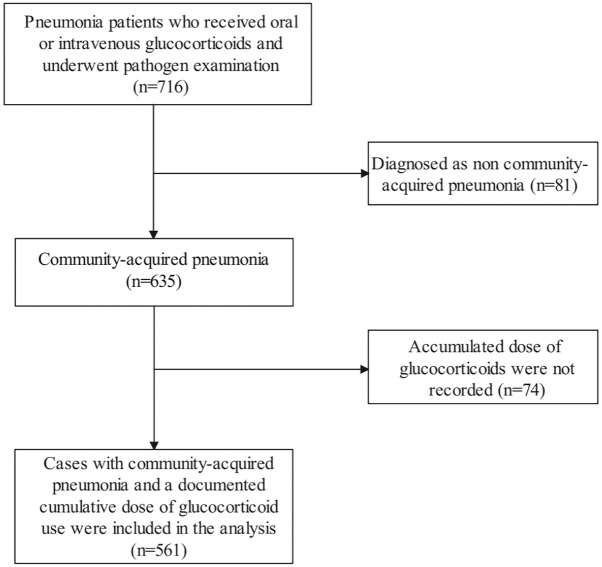
Methods: We examined data from 561 patients diagnosed with CAP who had received either oral or intravenous glucocorticoids prior to their CAP diagnosis. To evaluate the effect of CGD on mortality risk, we employed piecewise linear regression and Cox regression analyses, adjusting for relevant confounders.
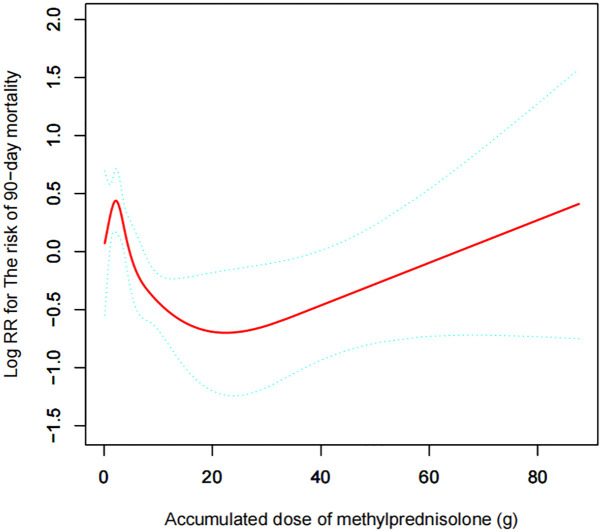
Results: Among the study population, the median CGD was 4 g of methylprednisolone (interquartile range 2.16-8.80 g). The 30-, 60-, and 90-day mortality rates were 22.28%, 25.13%, and 25.49%, respectively. Piecewise linear regression analysis revealed a nonlinear relationship between methylprednisolone dose and mortality risk, indicating a threshold effect at a methylprednisolone level of 20 g. In addition, Cox regression analysis showed a significantly higher mortality risk in patients with CGD exceeding 40 g of methylprednisolone compared to those with CGD between 20 and 40 g, after adjusting for potential confounding factors (adjusted HR 5.16, 95% CI: 1.16-22.99, p < 0.05).
Conclusion: CAP occurring in close proximity to recent high doses of steroids is associated with pathogens typically seen in immunocompromised hosts and is linked to higher mortality compared to usual CAP.
期刊介绍:
Therapeutic Advances in Respiratory Disease delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of respiratory disease.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


