Zaamin B Hussain, Sameer R Khawaja, Musab Gulzar, Hayden L Cooke, Krishna N Chopra, Robert S Roundy, Michael B Gottschalk, Eric R Wagner
{"title":"Glenoid Bone Grafting During Primary Reverse Shoulder Arthroplasty: A Learning-Curve Analysis.","authors":"Zaamin B Hussain, Sameer R Khawaja, Musab Gulzar, Hayden L Cooke, Krishna N Chopra, Robert S Roundy, Michael B Gottschalk, Eric R Wagner","doi":"10.2106/JBJS.OA.24.00125","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Reverse shoulder arthroplasty (RSA) with structural bone grafting of the glenoid utilizing an autograft from the resected humeral head is an effective strategy to address severe glenoid bone loss. Although learning curves have been established for RSA, RSA with bone grafting is more technically challenging, with relatively higher complication rates. The number of cases needed for proficiency and the optimal learning strategies have yet to be defined for RSA with bone grafting.</p><p><strong>Methods: </strong>All patients who underwent primary, single-stage RSA with bone grafting for severe glenoid bone loss at our institution between November 2018 and February 2022 were identified. Perioperative data, including imaging, operative time, complications, revisions, postoperative functional data, and patient-reported outcomes, were recorded and analyzed. The learning curve for a fellowship-trained shoulder and elbow surgeon was analyzed using linear regression and cumulative sum (CUSUM) analysis. CUSUM analysis objectively evaluated differences in operative time over the course of the surgeon's practice and elucidated the completion of the learning curve.</p><p><strong>Results: </strong>A total of 32 patients (53% male and 47% female; mean age, 68 years) were included in the analysis. The mean follow-up was 28 months. The mean operative time was 127 minutes, and there was a linear decrease in operative time throughout the study. CUSUM analysis using operative times demonstrated that the surgeon's learning curve was 14 patients. When comparing patients among the first 14 cases and the last 18 cases, there was no difference in shoulder range of motion, American Shoulder and Elbow Surgeons (ASES) scores, and Subjective Shoulder Value (SSV), while visual analog scale (VAS) pain scores at the time of final follow-up were better for patients in the surgeon's proficiency phase compared with the learning phase.</p><p><strong>Conclusions: </strong>In this study, we found a significant linear decrease in operative time with the number of cases completed, without associated detriment to the postoperative outcome or complication rate. Our findings suggest that at least 14 cases may be required before proficiency is obtained with RSA using humeral head bone graft.</p><p><strong>Level of evidence: </strong>Prognostic Level IV. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 2","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020699/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.24.00125","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
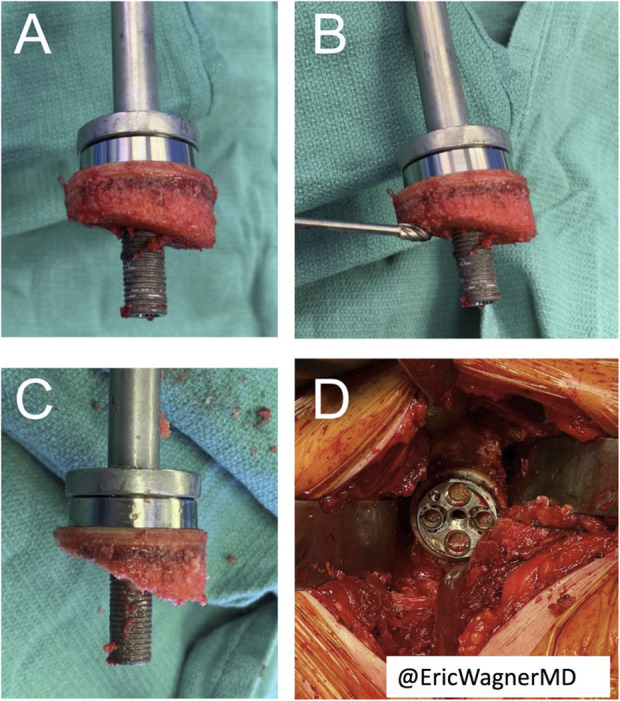
Background: Reverse shoulder arthroplasty (RSA) with structural bone grafting of the glenoid utilizing an autograft from the resected humeral head is an effective strategy to address severe glenoid bone loss. Although learning curves have been established for RSA, RSA with bone grafting is more technically challenging, with relatively higher complication rates. The number of cases needed for proficiency and the optimal learning strategies have yet to be defined for RSA with bone grafting.
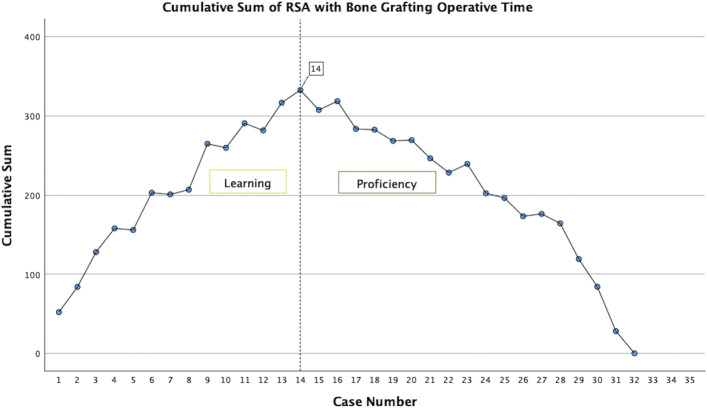
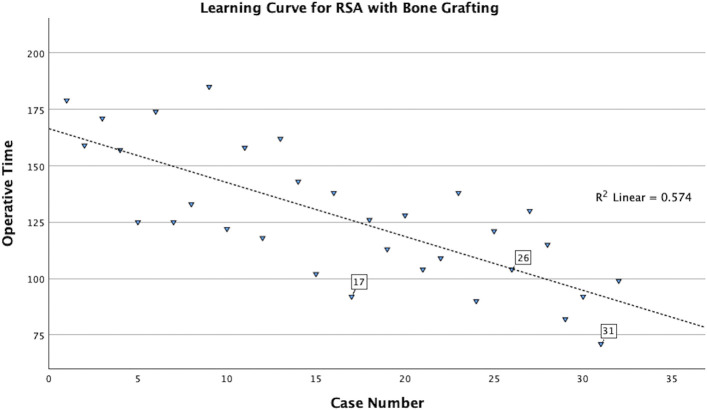
Methods: All patients who underwent primary, single-stage RSA with bone grafting for severe glenoid bone loss at our institution between November 2018 and February 2022 were identified. Perioperative data, including imaging, operative time, complications, revisions, postoperative functional data, and patient-reported outcomes, were recorded and analyzed. The learning curve for a fellowship-trained shoulder and elbow surgeon was analyzed using linear regression and cumulative sum (CUSUM) analysis. CUSUM analysis objectively evaluated differences in operative time over the course of the surgeon's practice and elucidated the completion of the learning curve.
Results: A total of 32 patients (53% male and 47% female; mean age, 68 years) were included in the analysis. The mean follow-up was 28 months. The mean operative time was 127 minutes, and there was a linear decrease in operative time throughout the study. CUSUM analysis using operative times demonstrated that the surgeon's learning curve was 14 patients. When comparing patients among the first 14 cases and the last 18 cases, there was no difference in shoulder range of motion, American Shoulder and Elbow Surgeons (ASES) scores, and Subjective Shoulder Value (SSV), while visual analog scale (VAS) pain scores at the time of final follow-up were better for patients in the surgeon's proficiency phase compared with the learning phase.
Conclusions: In this study, we found a significant linear decrease in operative time with the number of cases completed, without associated detriment to the postoperative outcome or complication rate. Our findings suggest that at least 14 cases may be required before proficiency is obtained with RSA using humeral head bone graft.
Level of evidence: Prognostic Level IV. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


