Marco Aurélio da Silva Neves, Lucas Leal Fraga, Moises Barbosa de Andrade, Bruno Ramos Nascimento, Cláudio Leo Gelape, Renato Bráulio, Paulo Henrique Nogueira Costa, Marcia Fabrícia Almeida Teixeira, Paulo Henrique Moreira Melo, Guilherme Rafael Sant'Anna Athayde, Lucas Lodi-Junqueira, Robert A Levine, Maria Carmo Pereira Nunes
{"title":"Clinical Outcomes After Valve Intervention in Rheumatic Mitral Valve Disease.","authors":"Marco Aurélio da Silva Neves, Lucas Leal Fraga, Moises Barbosa de Andrade, Bruno Ramos Nascimento, Cláudio Leo Gelape, Renato Bráulio, Paulo Henrique Nogueira Costa, Marcia Fabrícia Almeida Teixeira, Paulo Henrique Moreira Melo, Guilherme Rafael Sant'Anna Athayde, Lucas Lodi-Junqueira, Robert A Levine, Maria Carmo Pereira Nunes","doi":"10.5334/gh.1420","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rheumatic heart disease (RHD) remains one of the leading causes of mitral valve (MV) disease in developing countries. Despite the availability of percutaneous and surgical interventions, long-term outcomes remain unclear. This study aims to identify determinants of outcomes following percutaneous or surgical intervention in patients with rheumatic MV disease, addressing critical gaps in treatment selection.</p><p><strong>Methods: </strong>A retrospective, intention-to-treat study was conducted on patients with symptomatic rheumatic MV disease, primarily characterized by mitral stenosis, who underwent either percutaneous mitral valvuloplasty (PMV) or MV replacement (MVR). Demographic, clinical, and echocardiographic variables were collected. The long-term outcome was defined as a composite of death, repeat PMV, need for cardiac surgery, and stroke.</p><p><strong>Results: </strong>A total of 246 patients were enrolled (mean age 43.8 ± 13 years, 80% women, with 45% in New York Heart Association [NYHA] class III/IV). Of these, 90 patients (37%) underwent MVR, while 156 patients (63%) underwent PMV, with similar clinical characteristics at baseline. During a mean follow-up of 2.8 years, ranging from 1 day to 7.8 years, 45 patients (18%) reached the composite outcome, including 11 deaths (4%). Long-term outcomes were comparable between PMV and MVR (P = 0.231). Independent predictors of composite outcomes included baseline NYHA class III/IV (adjusted hazard ratio [HR] 2.10, 95% confidence interval [CI] 1.10-4.11, P = 0.023) and older age (HR 1.03, 95% CI 1.01-1.06, p = 0.020). Predictors of all-cause mortality following either PMV or MVR were older age (HR 1.08, 95% CI 1.03-1.14, P = 0.002) and lower left ventricular ejection fraction (HR 0.93, 95% CI 0.88-0.99, P = 0.021).</p><p><strong>Conclusions: </strong>This study identified older age and higher NYHA functional class as significant predictors of composite outcomes in patients with rheumatic MV disease requiring intervention. Left ventricular systolic dysfunction was independently associated with increased mortality following both percutaneous and surgical intervention. Long-term outcomes were comparable between patients undergoing PMV and MVR, reinforcing PMV as an effective alternative to surgery in appropriately selected patients.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"20 1","pages":"38"},"PeriodicalIF":3.1000,"publicationDate":"2025-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11987853/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1420","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Rheumatic heart disease (RHD) remains one of the leading causes of mitral valve (MV) disease in developing countries. Despite the availability of percutaneous and surgical interventions, long-term outcomes remain unclear. This study aims to identify determinants of outcomes following percutaneous or surgical intervention in patients with rheumatic MV disease, addressing critical gaps in treatment selection.
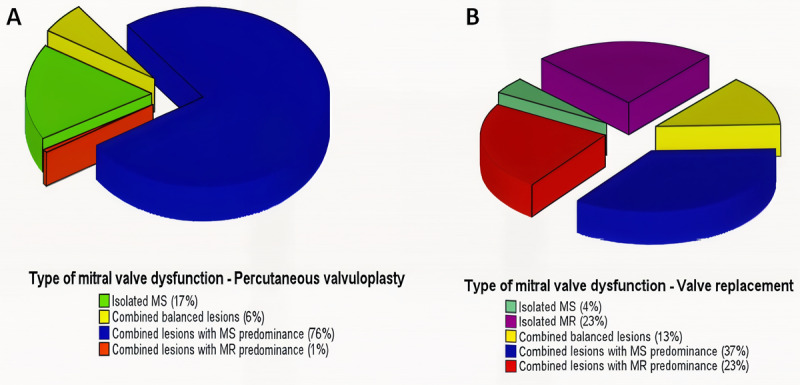
Methods: A retrospective, intention-to-treat study was conducted on patients with symptomatic rheumatic MV disease, primarily characterized by mitral stenosis, who underwent either percutaneous mitral valvuloplasty (PMV) or MV replacement (MVR). Demographic, clinical, and echocardiographic variables were collected. The long-term outcome was defined as a composite of death, repeat PMV, need for cardiac surgery, and stroke.
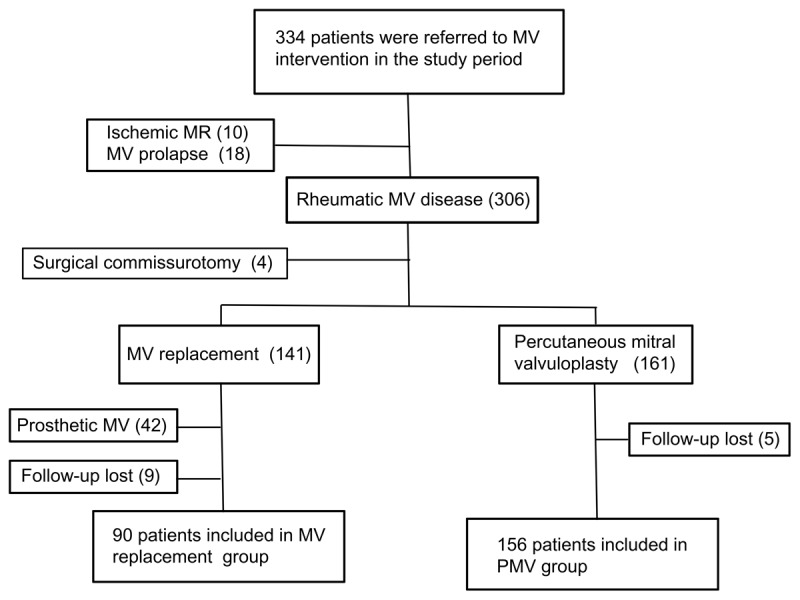
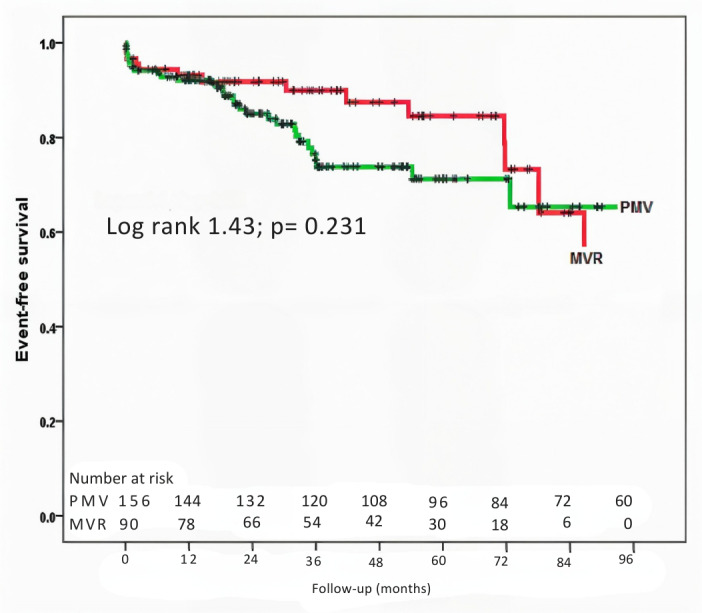
Results: A total of 246 patients were enrolled (mean age 43.8 ± 13 years, 80% women, with 45% in New York Heart Association [NYHA] class III/IV). Of these, 90 patients (37%) underwent MVR, while 156 patients (63%) underwent PMV, with similar clinical characteristics at baseline. During a mean follow-up of 2.8 years, ranging from 1 day to 7.8 years, 45 patients (18%) reached the composite outcome, including 11 deaths (4%). Long-term outcomes were comparable between PMV and MVR (P = 0.231). Independent predictors of composite outcomes included baseline NYHA class III/IV (adjusted hazard ratio [HR] 2.10, 95% confidence interval [CI] 1.10-4.11, P = 0.023) and older age (HR 1.03, 95% CI 1.01-1.06, p = 0.020). Predictors of all-cause mortality following either PMV or MVR were older age (HR 1.08, 95% CI 1.03-1.14, P = 0.002) and lower left ventricular ejection fraction (HR 0.93, 95% CI 0.88-0.99, P = 0.021).
Conclusions: This study identified older age and higher NYHA functional class as significant predictors of composite outcomes in patients with rheumatic MV disease requiring intervention. Left ventricular systolic dysfunction was independently associated with increased mortality following both percutaneous and surgical intervention. Long-term outcomes were comparable between patients undergoing PMV and MVR, reinforcing PMV as an effective alternative to surgery in appropriately selected patients.
背景:风湿性心脏病(RHD)仍然是发展中国家二尖瓣(MV)疾病的主要原因之一。尽管有经皮和手术干预,但长期结果尚不清楚。本研究旨在确定风湿MV患者经皮或手术干预后预后的决定因素,解决治疗选择中的关键空白。方法:对以二尖瓣狭窄为主要特征,行经皮二尖瓣成形术(PMV)或二尖瓣置换术(MVR)的有症状的风湿性二尖瓣疾病患者进行回顾性、意向治疗研究。收集了人口统计学、临床和超声心动图变量。长期结局定义为死亡、重复PMV、需要心脏手术和中风的综合结果。结果:共纳入246例患者(平均年龄43.8±13岁,80%为女性,45%为纽约心脏协会[NYHA] III/IV级)。其中,90例患者(37%)接受了MVR, 156例患者(63%)接受了PMV,在基线时具有相似的临床特征。在平均2.8年的随访期间,从1天到7.8年不等,45名患者(18%)达到复合结局,包括11例死亡(4%)。PMV和MVR的长期预后具有可比性(P = 0.231)。综合结果的独立预测因子包括基线NYHA III/IV级(校正风险比[HR] 2.10, 95%可信区间[CI] 1.10-4.11, P = 0.023)和年龄(HR 1.03, 95% CI 1.01-1.06, P = 0.020)。PMV或MVR后全因死亡率的预测因子为年龄较大(HR 1.08, 95% CI 1.03-1.14, P = 0.002)和较低的左室射血分数(HR 0.93, 95% CI 0.88-0.99, P = 0.021)。结论:本研究确定年龄较大和较高的NYHA功能分级是需要干预的风湿性中压病患者综合预后的重要预测因素。左心室收缩功能不全与经皮和手术干预后死亡率增加独立相关。接受PMV和MVR的患者之间的长期结果具有可比性,在适当选择的患者中,PMV作为手术的有效替代方案得到了加强。
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


