Microscopically-assisted Uninstrumented Surgical Tumor Decompression as an alternative to open surgery for symptomatic metastatic epidural spinal cord compression.
Camryn E Harvie, Richard J Chung, Sriyaa Suresh, John C O'Donnell, Alexander J Schupper, Arthur L Jenkins
{"title":"Microscopically-assisted Uninstrumented Surgical Tumor Decompression as an alternative to open surgery for symptomatic metastatic epidural spinal cord compression.","authors":"Camryn E Harvie, Richard J Chung, Sriyaa Suresh, John C O'Donnell, Alexander J Schupper, Arthur L Jenkins","doi":"10.21037/jss-24-135","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The current standard of care recommends spinal tumor decompression surgery prior to radiation. However, the differences in open <i>vs.</i> minimally invasive surgery (MIS), extent of vertebroplasty, and role of instrumentation remains unclear across the literature. This study aims to assess whether our proposed Microscopically-Assisted Uninstrumented Spinal Tumor Decompression (MUST-D) technique using vertebral augmentation (VA) offers a surgical advantage over standard open instrumented fusion in the treatment of symptomatic metastatic epidural spinal cord compression (MESCC).</p><p><strong>Methods: </strong>This single-institution retrospective cohort study evaluated patients who underwent either standard open decompression with instrumented fusion (Control) or MIS with vertebrectomy and cement augmentation (MUST-D) for MESCC decompression from November 2006 to June 2016. Demographic, surgical, and follow-up data were extracted from medical records. The inclusion criteria were radiographic evidence of MESCC, pathology-confirmed spinal metastasis, and symptoms of vertebral instability or neural compression. Outcomes included length of operation, anesthesia duration, estimated blood loss (EBL), hospital stay, complications, time until radiation therapy (RTx), Hauser Ambulation Index (HAI), Cobb angle, mortality, and survival.</p><p><strong>Results: </strong>Among 59 MESCC surgeries, 21 (36%) had MUST-D and 38 (64%) had open surgery (60.8 <i>vs.</i> 59.2 years, P=0.62). Preoperative Spine Instability Neoplastic Score (SINS) (P=0.40) and index level of surgery (P=0.44) were similar between groups. The MUST-D group had reduced length of operation (P<0.001), anesthesia duration (P=0.004), hospital stay (P=0.01) and complications (P<0.001) compared to the control group. Trends toward decreased EBL were observed (P=0.06). Postoperatively, the MUST-D group had shorter time to RTx compared to the control group (P=0.03). Despite similar pre-operative ambulation, the MUST-D group had a shorter time to ambulation postoperatively compared to the control group (0.41 <i>vs.</i> 3.68 days, P=0.02). Moreover, the MUST-D group demonstrated improvement in 30-day HAI ambulation score, whereas the control group worsened (-1.60 <i>vs.</i> 0.33, P=0.008). Both groups had improved Cobb angle, with no new instability or focal kyphosis across a mean follow-up period of 1.51 years. No differences were observed in 1-year mortality (P=0.16) or Kaplan-Meier survival estimates (P=0.18). However, of patients who died, the MUST-D group demonstrated a longer time to death (P=0.04).</p><p><strong>Conclusions: </strong>Our findings indicate that the MUST-D technique provides surgical advantages compared to standard open surgery for MESCC, with significant improvement in perioperative outcomes. Although both groups had similar 1-year mortality, the MUST-D cohort demonstrated shorter time to RTx, faster postoperative ambulation, improved 30-day ambulatory function, similar index level revision rates, and longer time to death compared to open procedures. With no inferior outcome recorded in our study, the MUST-D technique is observed as an improvement over standard approach. Thus, we propose the MUST-D technique as an alternative treatment modality for symptomatic MESCC decompression. Larger randomized prospective studies with robust clinical correlation are warranted to confirm these findings.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"11 1","pages":"74-87"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11998037/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-135","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The current standard of care recommends spinal tumor decompression surgery prior to radiation. However, the differences in open vs. minimally invasive surgery (MIS), extent of vertebroplasty, and role of instrumentation remains unclear across the literature. This study aims to assess whether our proposed Microscopically-Assisted Uninstrumented Spinal Tumor Decompression (MUST-D) technique using vertebral augmentation (VA) offers a surgical advantage over standard open instrumented fusion in the treatment of symptomatic metastatic epidural spinal cord compression (MESCC).
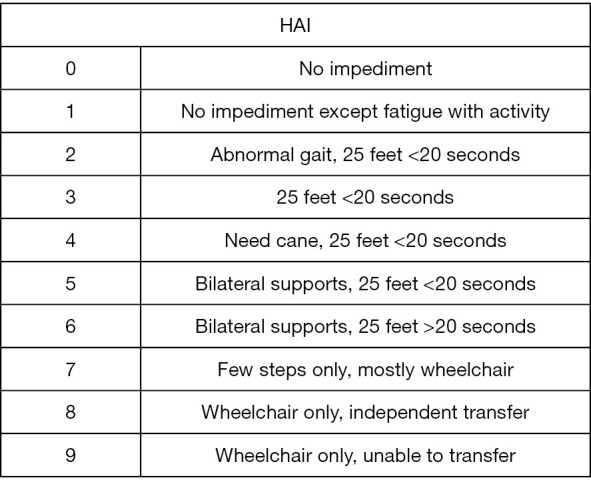
Methods: This single-institution retrospective cohort study evaluated patients who underwent either standard open decompression with instrumented fusion (Control) or MIS with vertebrectomy and cement augmentation (MUST-D) for MESCC decompression from November 2006 to June 2016. Demographic, surgical, and follow-up data were extracted from medical records. The inclusion criteria were radiographic evidence of MESCC, pathology-confirmed spinal metastasis, and symptoms of vertebral instability or neural compression. Outcomes included length of operation, anesthesia duration, estimated blood loss (EBL), hospital stay, complications, time until radiation therapy (RTx), Hauser Ambulation Index (HAI), Cobb angle, mortality, and survival.
Results: Among 59 MESCC surgeries, 21 (36%) had MUST-D and 38 (64%) had open surgery (60.8 vs. 59.2 years, P=0.62). Preoperative Spine Instability Neoplastic Score (SINS) (P=0.40) and index level of surgery (P=0.44) were similar between groups. The MUST-D group had reduced length of operation (P<0.001), anesthesia duration (P=0.004), hospital stay (P=0.01) and complications (P<0.001) compared to the control group. Trends toward decreased EBL were observed (P=0.06). Postoperatively, the MUST-D group had shorter time to RTx compared to the control group (P=0.03). Despite similar pre-operative ambulation, the MUST-D group had a shorter time to ambulation postoperatively compared to the control group (0.41 vs. 3.68 days, P=0.02). Moreover, the MUST-D group demonstrated improvement in 30-day HAI ambulation score, whereas the control group worsened (-1.60 vs. 0.33, P=0.008). Both groups had improved Cobb angle, with no new instability or focal kyphosis across a mean follow-up period of 1.51 years. No differences were observed in 1-year mortality (P=0.16) or Kaplan-Meier survival estimates (P=0.18). However, of patients who died, the MUST-D group demonstrated a longer time to death (P=0.04).
Conclusions: Our findings indicate that the MUST-D technique provides surgical advantages compared to standard open surgery for MESCC, with significant improvement in perioperative outcomes. Although both groups had similar 1-year mortality, the MUST-D cohort demonstrated shorter time to RTx, faster postoperative ambulation, improved 30-day ambulatory function, similar index level revision rates, and longer time to death compared to open procedures. With no inferior outcome recorded in our study, the MUST-D technique is observed as an improvement over standard approach. Thus, we propose the MUST-D technique as an alternative treatment modality for symptomatic MESCC decompression. Larger randomized prospective studies with robust clinical correlation are warranted to confirm these findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


