Association of Diaphragmatic Mobility and Thickening Fraction with Postoperative Pulmonary Complications in Patients Undergoing Thoracic Surgery and Their Application in Prediction.
IF 2.8 3区 医学Q1 Pharmacology, Toxicology and Pharmaceutics
{"title":"Association of Diaphragmatic Mobility and Thickening Fraction with Postoperative Pulmonary Complications in Patients Undergoing Thoracic Surgery and Their Application in Prediction.","authors":"Abudushalamu Aisiaiti, Aiwuzaili Ajiaikebaier, Aini Maimaitiming, Qiang Geng, Bichen He, Jinhui Sun, Bing Zhang","doi":"10.2147/TCRM.S519646","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To investigate the association of diaphragmatic mobility and thickening fraction with postoperative pulmonary complications (PPCs) in patients undergoing thoracic surgery and evaluate their values in predicting PPCs.</p><p><strong>Patients and methods: </strong>One hundred and nine consecutive patients undergoing thoracic surgery were prospectively enrolled. All patients underwent ultrasound measurements to obtain diaphragmatic mobility and thickening fraction. PPCs were systematically monitored and recorded from postoperative day 1 to 7. The binary logistic regression model was used to perform multivariate analysis, and the receiver operating characteristic (ROC) curve was used to evaluate predictive values.</p><p><strong>Results: </strong>PPCs occurred in 46 patients (42.2%). Multivariate analysis identified age, smoking, surgical sites, and mean diaphragmatic mobility and thickening fraction of operated side and nonoperated side as independent risk factors for PPCs. ROC curves revealed that the AUC of mean diaphragmatic mobility and thickening fraction for predicting PPCs in patients undergoing thoracic surgery was 0.722 [standard error (<i>SE</i>): 0.050, 95% confidence interval (<i>CI</i>): 0.623~0.821, <i>P</i><0.001] and 0.757 (<i>SE</i>: 0.050, 95% <i>CI</i>: 0.659~0.855, <i>P</i><0.001), respectively. The predictive model integrating age, smoking and surgical sites yielded an AUC of 0.810 (<i>SE</i>: 0.041, 95% <i>CI</i>: 0.728~0.891, <i>P</i><0.001), while the predictive model integrating age, smoking, surgical sites and mean diaphragmatic mobility or thickening fraction yielded an AUC of 0.849 (<i>SE</i>: 0.037, 95% <i>CI</i>: 0.777~0.922, <i>P</i><0.001) and 0.881 (<i>SE</i>: 0.033, 95% <i>CI</i>: 0.815~0.946, <i>P</i><0.001), respectively.</p><p><strong>Conclusion: </strong>Both diaphragmatic mobility and thickening fraction showed independent associations with PPCs following thoracic surgery, demonstrating moderate predictive values. The predictive models integrating age, smoking, surgical sites and diaphragmatic mobility or thickening fraction yielded high predictive values, suggesting significant clinical utility for risk stratification. Diaphragmatic mobility and thickening fraction offer a bedside, noninvasive, and cost-effective alternative for perioperative PPC prediction, particularly in resource-limited settings.</p>","PeriodicalId":22977,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"21 ","pages":"501-509"},"PeriodicalIF":2.8000,"publicationDate":"2025-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12035405/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S519646","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To investigate the association of diaphragmatic mobility and thickening fraction with postoperative pulmonary complications (PPCs) in patients undergoing thoracic surgery and evaluate their values in predicting PPCs.
Patients and methods: One hundred and nine consecutive patients undergoing thoracic surgery were prospectively enrolled. All patients underwent ultrasound measurements to obtain diaphragmatic mobility and thickening fraction. PPCs were systematically monitored and recorded from postoperative day 1 to 7. The binary logistic regression model was used to perform multivariate analysis, and the receiver operating characteristic (ROC) curve was used to evaluate predictive values.
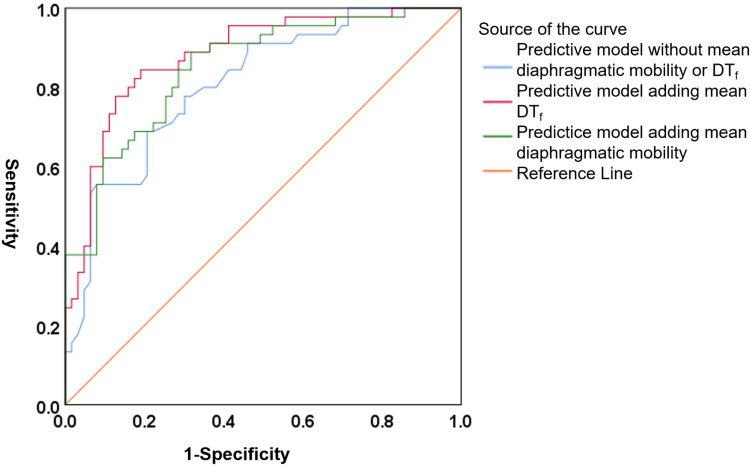
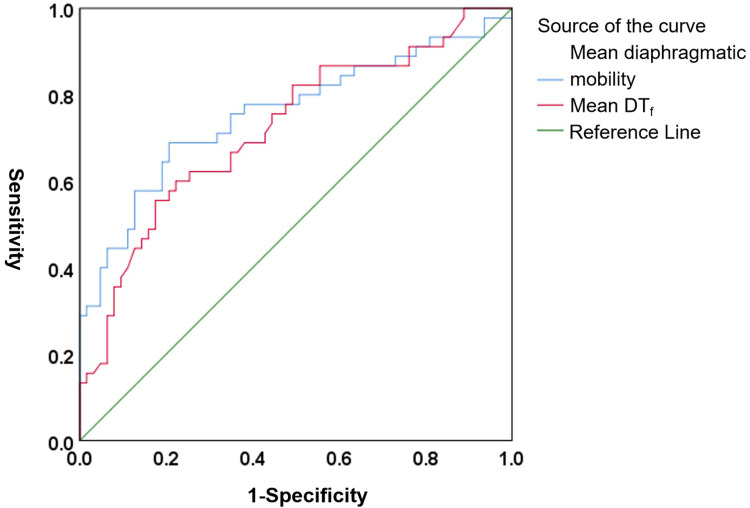
Results: PPCs occurred in 46 patients (42.2%). Multivariate analysis identified age, smoking, surgical sites, and mean diaphragmatic mobility and thickening fraction of operated side and nonoperated side as independent risk factors for PPCs. ROC curves revealed that the AUC of mean diaphragmatic mobility and thickening fraction for predicting PPCs in patients undergoing thoracic surgery was 0.722 [standard error (SE): 0.050, 95% confidence interval (CI): 0.623~0.821, P<0.001] and 0.757 (SE: 0.050, 95% CI: 0.659~0.855, P<0.001), respectively. The predictive model integrating age, smoking and surgical sites yielded an AUC of 0.810 (SE: 0.041, 95% CI: 0.728~0.891, P<0.001), while the predictive model integrating age, smoking, surgical sites and mean diaphragmatic mobility or thickening fraction yielded an AUC of 0.849 (SE: 0.037, 95% CI: 0.777~0.922, P<0.001) and 0.881 (SE: 0.033, 95% CI: 0.815~0.946, P<0.001), respectively.
Conclusion: Both diaphragmatic mobility and thickening fraction showed independent associations with PPCs following thoracic surgery, demonstrating moderate predictive values. The predictive models integrating age, smoking, surgical sites and diaphragmatic mobility or thickening fraction yielded high predictive values, suggesting significant clinical utility for risk stratification. Diaphragmatic mobility and thickening fraction offer a bedside, noninvasive, and cost-effective alternative for perioperative PPC prediction, particularly in resource-limited settings.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


