Association of central capillary refill time with mortality in adult trauma patients: a secondary analysis of the crash-2 randomised controlled trial data.
Sabrina Jegerlehner, Tim Harris, Martin Mueller, Ben Bloom
{"title":"Association of central capillary refill time with mortality in adult trauma patients: a secondary analysis of the crash-2 randomised controlled trial data.","authors":"Sabrina Jegerlehner, Tim Harris, Martin Mueller, Ben Bloom","doi":"10.1186/s13049-025-01407-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Trauma-related injuries account for up to 4.4 million deaths annually worldwide. Failure to identify haemorrhage in trauma patients increases mortality. This study examines the association of central capillary refill time (CRT) and mortality in adult trauma patients, especially in the subgroup with normal heart rate (HR) and blood pressure (BP).</p><p><strong>Methods: </strong>This retrospective observational study analysed data from the CRASH-2 trial, conducted in 274 hospitals across 40 countries and 5 continents between May 2005 and January 2010. A total of 19,054 out of 20,207 adult trauma patients with recorded CRT and complete dataset were included. CRT was taken centrally (sternum) and categorized as ≤ 2, 3-4, and ≥ 5 s. The primary outcome was 28-day mortality, while secondary outcomes included need for transfusion, surgical intervention and thromboembolic events. Univariable and multivariable logistic regression analysis were conducted, incorporating random effects for continent/cluster. Receiver operating characteristic curves were used to assess the discriminatory ability of central CRT measurement.</p><p><strong>Results: </strong>Among the patients, 6,756 (35.5%) had a CRT ≤ 2 s, 9,142 (48%) had a CRT of 3-4 s, and 3,156 (16.6%) had a CRT ≥ 5 s. Compared to the reference category (CRT ≤ 2 s), the odds of death were significantly higher in patients with CRT of 3-4 s (OR 1.7, 95% CI 1.6-1.9) and CRT ≥ 5 s (OR 3.2, 95% CI 2.8-3.5). Higher CRT was also associated with an increased likelihood of blood transfusion, surgical intervention, and thromboembolic events. The AUC values ranged from 0.63 to 0.74 and were consistent with a significant association between the variables.</p><p><strong>Conclusion: </strong>Central CRT is associated with increased mortality and adverse outcomes in trauma patients. In bleeding trauma patients, an increasing central CRT is linked to higher mortality risk, with a central CRT ≥ 5 s being particularly predictive of worse outcomes. This also applies to patients with stable vital signs (normal HR and BP), suggesting that CRT may offer additional value as an indicator of hidden hypoperfusion.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"82"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12070708/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01407-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Trauma-related injuries account for up to 4.4 million deaths annually worldwide. Failure to identify haemorrhage in trauma patients increases mortality. This study examines the association of central capillary refill time (CRT) and mortality in adult trauma patients, especially in the subgroup with normal heart rate (HR) and blood pressure (BP).
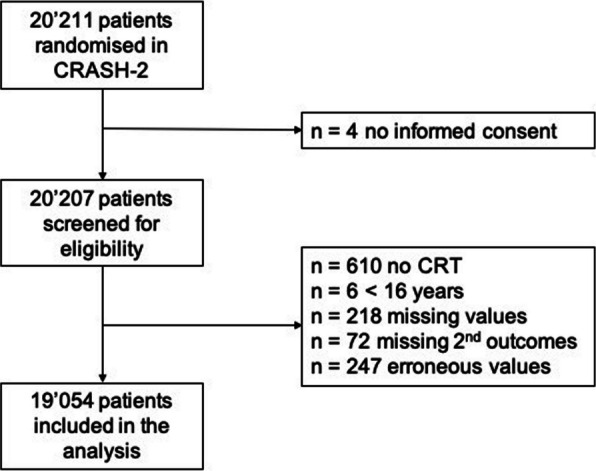
Methods: This retrospective observational study analysed data from the CRASH-2 trial, conducted in 274 hospitals across 40 countries and 5 continents between May 2005 and January 2010. A total of 19,054 out of 20,207 adult trauma patients with recorded CRT and complete dataset were included. CRT was taken centrally (sternum) and categorized as ≤ 2, 3-4, and ≥ 5 s. The primary outcome was 28-day mortality, while secondary outcomes included need for transfusion, surgical intervention and thromboembolic events. Univariable and multivariable logistic regression analysis were conducted, incorporating random effects for continent/cluster. Receiver operating characteristic curves were used to assess the discriminatory ability of central CRT measurement.
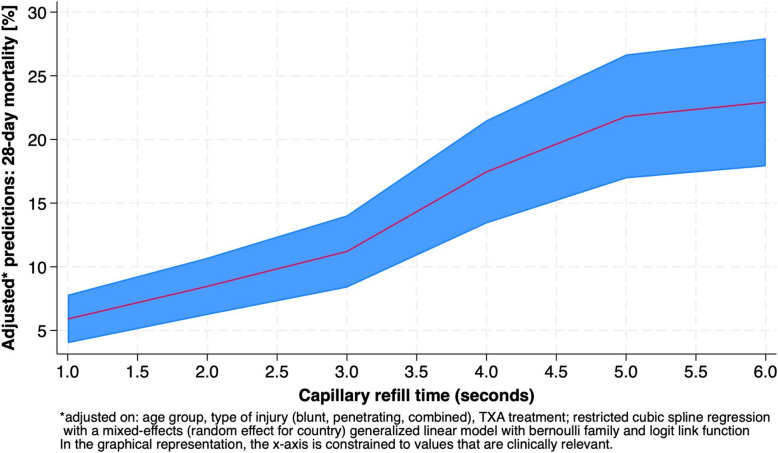
Results: Among the patients, 6,756 (35.5%) had a CRT ≤ 2 s, 9,142 (48%) had a CRT of 3-4 s, and 3,156 (16.6%) had a CRT ≥ 5 s. Compared to the reference category (CRT ≤ 2 s), the odds of death were significantly higher in patients with CRT of 3-4 s (OR 1.7, 95% CI 1.6-1.9) and CRT ≥ 5 s (OR 3.2, 95% CI 2.8-3.5). Higher CRT was also associated with an increased likelihood of blood transfusion, surgical intervention, and thromboembolic events. The AUC values ranged from 0.63 to 0.74 and were consistent with a significant association between the variables.
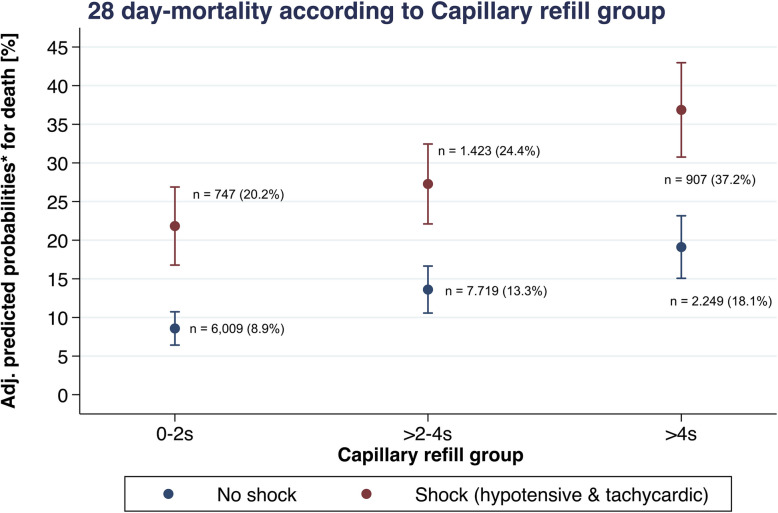
Conclusion: Central CRT is associated with increased mortality and adverse outcomes in trauma patients. In bleeding trauma patients, an increasing central CRT is linked to higher mortality risk, with a central CRT ≥ 5 s being particularly predictive of worse outcomes. This also applies to patients with stable vital signs (normal HR and BP), suggesting that CRT may offer additional value as an indicator of hidden hypoperfusion.
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


