{"title":"Kidney Outcomes with Corticosteroid Treatment in IgA Nephropathy According to the Oxford-MEST-C Classification.","authors":"Bancha Satirapoj, Thapana Chueaboonchai, Naowanit Nata, Ouppatham Supasyndh","doi":"10.1159/000545382","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Despite optimization of renin-angiotensin-aldosterone system (RAAS) inhibition, patients with IgA nephropathy remain at risk for kidney failure. The effect of steroids on kidney outcomes in IgA nephropathy with different renal pathologic lesions has been uncertain.</p><p><strong>Objective: </strong>This study aimed to evaluate the efficacy of steroid treatment in IgA nephropathy patients classified according to the Oxford-MEST-C classification.</p><p><strong>Methods: </strong>We retrospectively studied 67 patients with biopsy-proven IgA nephropathy who were receiving optimized RAAS inhibitor therapy and had persistent proteinuria >1 g/day between January 2016 and December 2020. Clinical parameters, including estimated glomerular filtration rate (GFR) decline, were compared between the corticosteroid and supportive treatment groups.</p><p><strong>Results: </strong>Overall, 68.7% of patients received treatment with corticosteroids. The median estimated GFR decline was significantly lower in the steroid group compared to the controls {-0.65 (interquartile range [IQR] -3.45 to 7) vs. -5.75 (IQR -10.65 to -0.7) mL/min/1.73 m<sup>2</sup>/year, <i>p</i> = 0.025}. The slope of estimated GFR was also significantly different between the steroid and control groups in patients with a baseline GFR >50 mL/min/1.73 m<sup>2</sup> (3.90 ± 11.42 vs. -9.31 ± 5.08 mL/min/1.73 m<sup>2</sup>/year, <i>p</i> = 0.011), mesangial hypercellularity M0 score (4.69 ± 11.37 vs. -2.63 ± 6.42 mL/min/1.73 m<sup>2</sup>/year, <i>p</i> = 0.049), and C0 score (2.48 ± 12.63 vs. -5.58 ± 8.4 mL/min/1.73 m<sup>2</sup>/year, <i>p</i> = 0.026). Additionally, rapid GFR decline (>5 mL/min/1.73 m<sup>2</sup>/year) occurred in 9 patients (19.6%) in the steroid group compared with 11 participants (52.4%) in the control group (<i>p</i> = 0.006).</p><p><strong>Conclusion: </strong>Corticosteroid therapy, in addition to optimized RAAS inhibition, lowers the risk of kidney disease progression in patients with IgA nephropathy, particularly those with a baseline GFR >50 mL/min/1.73 m<sup>2</sup> and those classified with Oxford scores M0 and C0.</p>","PeriodicalId":73177,"journal":{"name":"Glomerular diseases","volume":"5 1","pages":"191-199"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12043279/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Glomerular diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545382","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Despite optimization of renin-angiotensin-aldosterone system (RAAS) inhibition, patients with IgA nephropathy remain at risk for kidney failure. The effect of steroids on kidney outcomes in IgA nephropathy with different renal pathologic lesions has been uncertain.
Objective: This study aimed to evaluate the efficacy of steroid treatment in IgA nephropathy patients classified according to the Oxford-MEST-C classification.
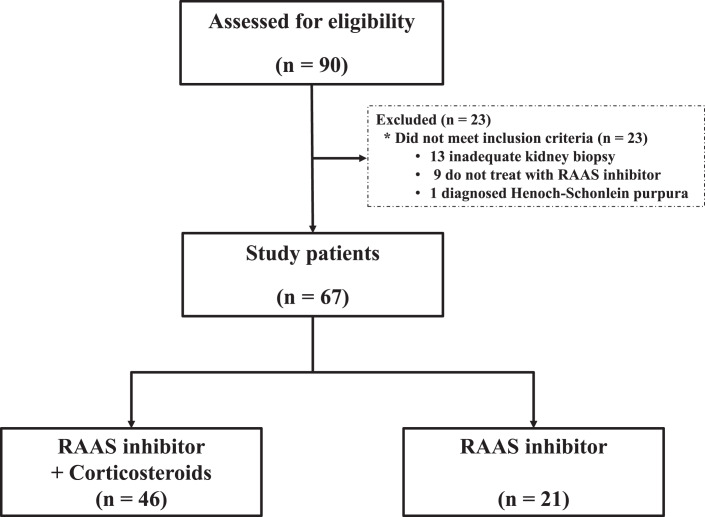
Methods: We retrospectively studied 67 patients with biopsy-proven IgA nephropathy who were receiving optimized RAAS inhibitor therapy and had persistent proteinuria >1 g/day between January 2016 and December 2020. Clinical parameters, including estimated glomerular filtration rate (GFR) decline, were compared between the corticosteroid and supportive treatment groups.
Results: Overall, 68.7% of patients received treatment with corticosteroids. The median estimated GFR decline was significantly lower in the steroid group compared to the controls {-0.65 (interquartile range [IQR] -3.45 to 7) vs. -5.75 (IQR -10.65 to -0.7) mL/min/1.73 m2/year, p = 0.025}. The slope of estimated GFR was also significantly different between the steroid and control groups in patients with a baseline GFR >50 mL/min/1.73 m2 (3.90 ± 11.42 vs. -9.31 ± 5.08 mL/min/1.73 m2/year, p = 0.011), mesangial hypercellularity M0 score (4.69 ± 11.37 vs. -2.63 ± 6.42 mL/min/1.73 m2/year, p = 0.049), and C0 score (2.48 ± 12.63 vs. -5.58 ± 8.4 mL/min/1.73 m2/year, p = 0.026). Additionally, rapid GFR decline (>5 mL/min/1.73 m2/year) occurred in 9 patients (19.6%) in the steroid group compared with 11 participants (52.4%) in the control group (p = 0.006).
Conclusion: Corticosteroid therapy, in addition to optimized RAAS inhibition, lowers the risk of kidney disease progression in patients with IgA nephropathy, particularly those with a baseline GFR >50 mL/min/1.73 m2 and those classified with Oxford scores M0 and C0.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


