{"title":"Severe Hypercalcemia Associated With Perinatal Hypophosphatasia While Receiving Enzyme Replacement Therapy.","authors":"Mostafa Salama, Alaa Al Nofal, Peter Tebben","doi":"10.1210/jcemcr/luaf066","DOIUrl":null,"url":null,"abstract":"<p><p>Hypophosphatasia (HPP) is characterized by defective bone mineralization due to reduced function of tissue-nonspecific alkaline phosphatase (TNSALP) caused by pathogenic <i>ALPL</i> gene variants. Hypercalcemia is more common in the perinatal and infantile forms and may be mitigated or prevented with enzyme replacement therapy asfotase alfa (AA). Here, we report a patient who developed severe hypercalcemia while receiving AA. Hypercalcemia was initially managed with intravenous fluids, dietary calcium restriction, and maximizing AA dose. Despite these measures, she required an additional hospital admission, at which time calcitonin 4 IU/kg every 12 hours was initiated. On this regimen, her calcium normalized without recurrence of severe hypercalcemia. Over the subsequent 8 months, restrictions of calcium intake were slowly lifted, and calcitonin was tapered and discontinued with maintenance of calcium within the normal range. This case underscores the significance of vigilant monitoring of calcium levels and dietary intake in infants diagnosed with HPP. While calcitonin is typically not considered as a sustained treatment for hypercalcemia, the present case illustrates the efficacy of adjunct calcitonin therapy, in conjunction with restricted calcium intake and maximum AA dosing, in managing severe hypercalcemia in an infant with perinatal HPP.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"3 5","pages":"luaf066"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11997545/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luaf066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
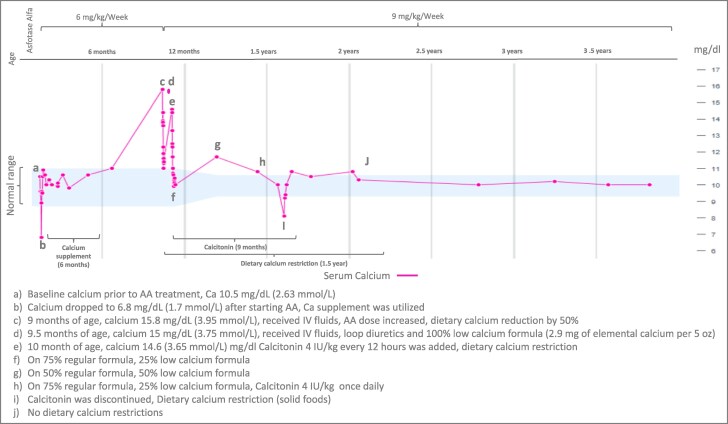
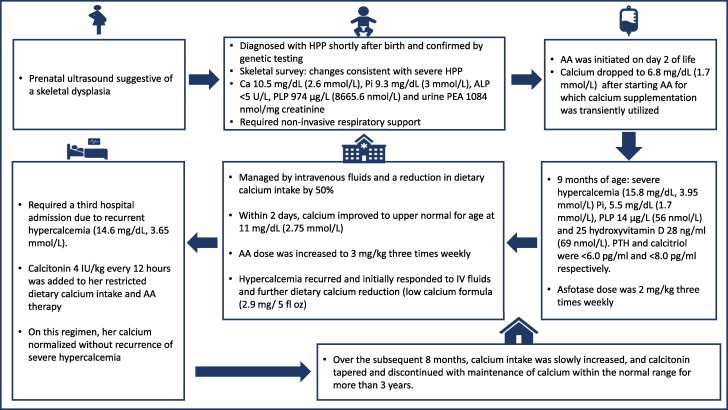
Hypophosphatasia (HPP) is characterized by defective bone mineralization due to reduced function of tissue-nonspecific alkaline phosphatase (TNSALP) caused by pathogenic ALPL gene variants. Hypercalcemia is more common in the perinatal and infantile forms and may be mitigated or prevented with enzyme replacement therapy asfotase alfa (AA). Here, we report a patient who developed severe hypercalcemia while receiving AA. Hypercalcemia was initially managed with intravenous fluids, dietary calcium restriction, and maximizing AA dose. Despite these measures, she required an additional hospital admission, at which time calcitonin 4 IU/kg every 12 hours was initiated. On this regimen, her calcium normalized without recurrence of severe hypercalcemia. Over the subsequent 8 months, restrictions of calcium intake were slowly lifted, and calcitonin was tapered and discontinued with maintenance of calcium within the normal range. This case underscores the significance of vigilant monitoring of calcium levels and dietary intake in infants diagnosed with HPP. While calcitonin is typically not considered as a sustained treatment for hypercalcemia, the present case illustrates the efficacy of adjunct calcitonin therapy, in conjunction with restricted calcium intake and maximum AA dosing, in managing severe hypercalcemia in an infant with perinatal HPP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


