Long-term outcomes of out-of-center veno-arterial ECMO cannulation for cardiopulmonary failure: investigation of prognostic parameters for a decision support tool - a 16-year retrospective study.
Walter Petermichl, Alois Philipp, Maik Foltan, Andrea Stadlbauer, Peter-Paul Ellmauer, Christian Merten, Sebastian Blecha, Thomas Müller, Bernhard Ulm, Bernhard Graf, Dirk Lunz
{"title":"Long-term outcomes of out-of-center veno-arterial ECMO cannulation for cardiopulmonary failure: investigation of prognostic parameters for a decision support tool - a 16-year retrospective study.","authors":"Walter Petermichl, Alois Philipp, Maik Foltan, Andrea Stadlbauer, Peter-Paul Ellmauer, Christian Merten, Sebastian Blecha, Thomas Müller, Bernhard Ulm, Bernhard Graf, Dirk Lunz","doi":"10.1186/s13049-025-01401-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Veno-arterial extracorporeal membrane oxygenation (VA ECMO) has served as a crucial intervention for critically ill patients with persistent cardiopulmonary failure. A standardized approach improves VA ECMO outcomes, which is why ECMO is currently limited to specialized centers. However, transferring critically ill patients to these ECMO centers is not without risk. Portable ECMO devices allow implantation in out-of-center settings prior to transportation. Despite efforts to standardize decision-making, significant variability remains, particularly in out-of-center (OoC) settings with limited data. Due to persistently high mortality, accurate indications are needed to optimize outcomes. This study aims to identify key factors associated with favorable outcomes in OoC VA ECMO and to develop practical decision-making tools for clinicians in these settings.</p><p><strong>Methods: </strong>We retrospectively investigated the outcomes of VA ECMO implantation in out-of-center settings between 2006 and 2022 at our institution. Parameters assessed prior to VA ECMO implantation, including organ failure count, mean arterial pressure (MAP), and laboratory data, were analyzed. Follow-up data were collected to evaluate functional (Eastern Cooperative Oncology Group [ECOG] performance status) and neurological (cerebral performance category score [CPC]) (outcomes. Statistical analyses were performed using non-parametric methods and SHAP importance analysis.</p><p><strong>Results: </strong>A total of 56.5% (195 of 345 patients) who underwent VA ECMO implantation in OoC survived, and 43.8% had a favorable neurological outcome (CPC 1). 37.6% of patients had good functional outcomes (ECOG 0-1). Patients with a MAP > 54 mmHg had better long-term functional outcomes, and those with a MAP > 64 mmHg had better mid-term neurological outcomes. Poor outcomes were associated with reduced coagulation activity and increased thrombogenicity. Renal and multi-organ failure prior to VA ECMO implantation were associated with poor neurological and functional outcomes.</p><p><strong>Conclusions: </strong>Through importance analyses, we identified key and secondary factors associated with favorable outcomes in OoC VA ECMO. The extent and severity of organ failure prior to VA ECMO implantation are crucial in determining outcomes. Hemodynamic status, as reflected by MAP, along with organ failure prior to VA-ECMO implantation, significantly influences neurological and functional outcomes. Patients with better hemodynamic stability and coagulation profiles had significantly improved chances of survival with favorable neurological and functional outcomes.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"81"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12070683/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01401-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Veno-arterial extracorporeal membrane oxygenation (VA ECMO) has served as a crucial intervention for critically ill patients with persistent cardiopulmonary failure. A standardized approach improves VA ECMO outcomes, which is why ECMO is currently limited to specialized centers. However, transferring critically ill patients to these ECMO centers is not without risk. Portable ECMO devices allow implantation in out-of-center settings prior to transportation. Despite efforts to standardize decision-making, significant variability remains, particularly in out-of-center (OoC) settings with limited data. Due to persistently high mortality, accurate indications are needed to optimize outcomes. This study aims to identify key factors associated with favorable outcomes in OoC VA ECMO and to develop practical decision-making tools for clinicians in these settings.
Methods: We retrospectively investigated the outcomes of VA ECMO implantation in out-of-center settings between 2006 and 2022 at our institution. Parameters assessed prior to VA ECMO implantation, including organ failure count, mean arterial pressure (MAP), and laboratory data, were analyzed. Follow-up data were collected to evaluate functional (Eastern Cooperative Oncology Group [ECOG] performance status) and neurological (cerebral performance category score [CPC]) (outcomes. Statistical analyses were performed using non-parametric methods and SHAP importance analysis.
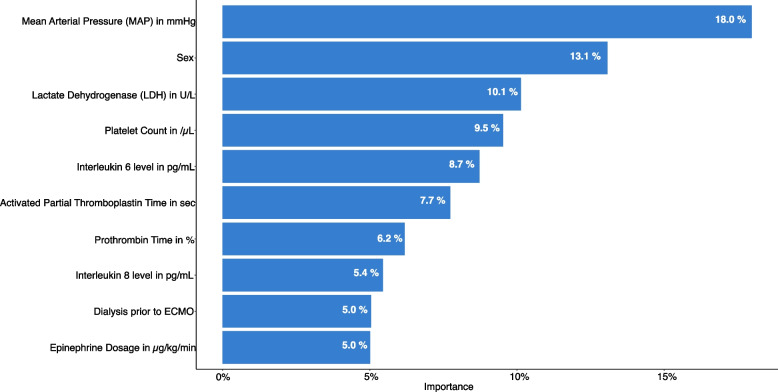
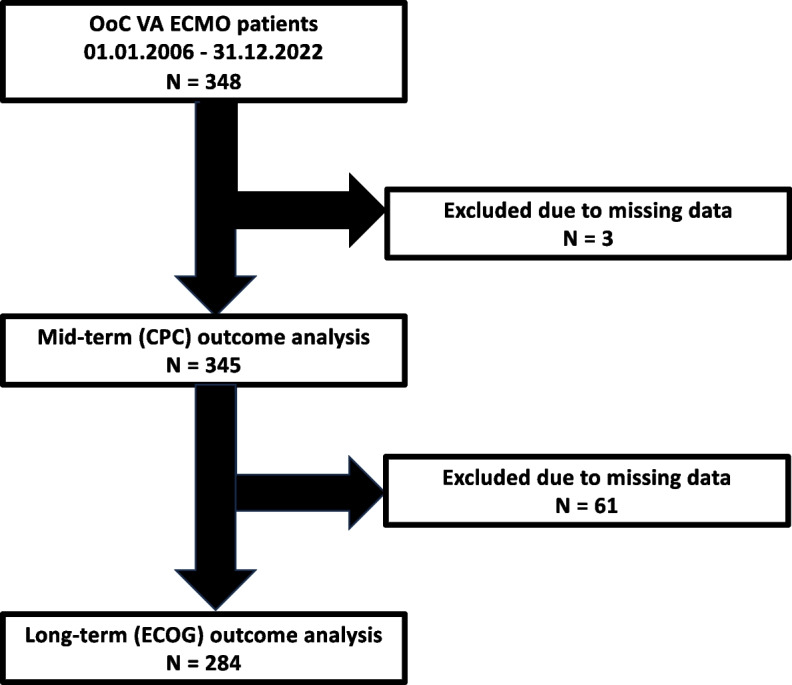
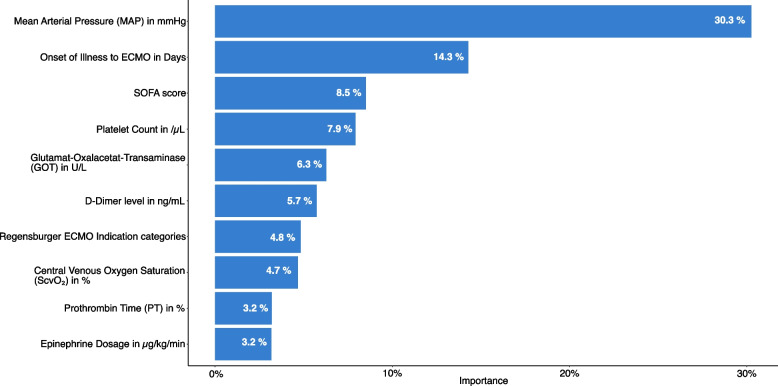
Results: A total of 56.5% (195 of 345 patients) who underwent VA ECMO implantation in OoC survived, and 43.8% had a favorable neurological outcome (CPC 1). 37.6% of patients had good functional outcomes (ECOG 0-1). Patients with a MAP > 54 mmHg had better long-term functional outcomes, and those with a MAP > 64 mmHg had better mid-term neurological outcomes. Poor outcomes were associated with reduced coagulation activity and increased thrombogenicity. Renal and multi-organ failure prior to VA ECMO implantation were associated with poor neurological and functional outcomes.
Conclusions: Through importance analyses, we identified key and secondary factors associated with favorable outcomes in OoC VA ECMO. The extent and severity of organ failure prior to VA ECMO implantation are crucial in determining outcomes. Hemodynamic status, as reflected by MAP, along with organ failure prior to VA-ECMO implantation, significantly influences neurological and functional outcomes. Patients with better hemodynamic stability and coagulation profiles had significantly improved chances of survival with favorable neurological and functional outcomes.
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


