Ellie Kelepouris, Nihar Desai, Katherine A A Clark, Mikhail N Kosiborod, Jeffrey Budden, Sandra Waechter, Michael Böhm
{"title":"Collaborative Management of Hyperkalemia in Patients with Complex Heart Failure.","authors":"Ellie Kelepouris, Nihar Desai, Katherine A A Clark, Mikhail N Kosiborod, Jeffrey Budden, Sandra Waechter, Michael Böhm","doi":"10.1159/000543931","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The aim of this study was to highlight the benefits and provide a framework for integrated multispecialty team involvement in the management of hyperkalemia in patients with heart failure (HF) and kidney disease and to ensure that patients receive optimal medical therapy to improve their clinical outcomes.</p><p><strong>Case presentation: </strong>This report highlights a hypothetical \"complex\" case of a patient with an acute HF decompensation who experiences hyperkalemia following up-titration of renin-angiotensin-aldosterone system inhibitor (RAASi) therapy. Two hypothetical scenarios for treatment management are discussed; in the first, providers down-titrate guideline-directed RAASi to avoid hyperkalemia, whereas in the second, providers take a collaborative interdisciplinary approach to manage hyperkalemia directly with the aim of avoiding RAASi down-titration. In the first typical management scenario, down-titration of guideline-directed RAASi to prevent increases in serum potassium (serum K<sup>+</sup>) levels leads to the reoccurrence of symptoms and rehospitalization of the patient. In the second proposed management scenario, interdisciplinary team discussions around differing tolerances and approaches to raised serum K<sup>+</sup> levels lead to maintenance of guideline-directed RAASi doses with the help of close monitoring of the patient, introduction of a low potassium diet, and prescription of potassium binder therapy.</p><p><strong>Conclusion: </strong>Collaborative multispecialty team management of HF patients may enable successful management of hyperkalemia without the need for discontinuation of guideline-directed RAASi therapy. Collaboration could extend to regular virtual or face-to-face cardiorenal clinics, where complex cases can be discussed, and local guidelines and processes can be developed.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"15 1","pages":"47-52"},"PeriodicalIF":0.9000,"publicationDate":"2025-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11999659/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543931","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The aim of this study was to highlight the benefits and provide a framework for integrated multispecialty team involvement in the management of hyperkalemia in patients with heart failure (HF) and kidney disease and to ensure that patients receive optimal medical therapy to improve their clinical outcomes.
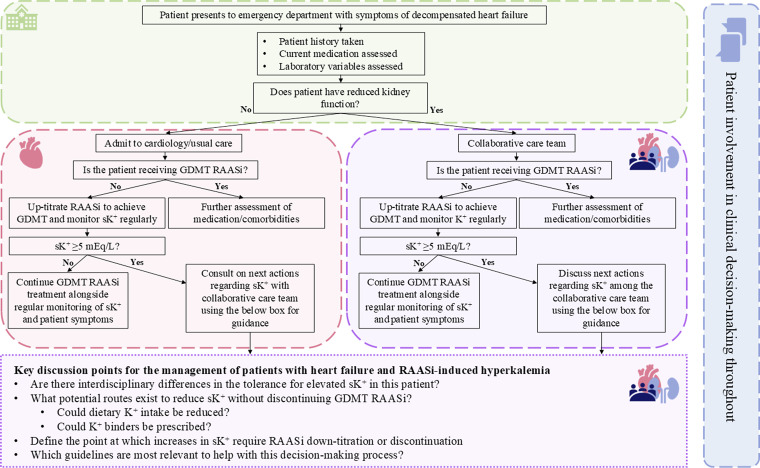
Case presentation: This report highlights a hypothetical "complex" case of a patient with an acute HF decompensation who experiences hyperkalemia following up-titration of renin-angiotensin-aldosterone system inhibitor (RAASi) therapy. Two hypothetical scenarios for treatment management are discussed; in the first, providers down-titrate guideline-directed RAASi to avoid hyperkalemia, whereas in the second, providers take a collaborative interdisciplinary approach to manage hyperkalemia directly with the aim of avoiding RAASi down-titration. In the first typical management scenario, down-titration of guideline-directed RAASi to prevent increases in serum potassium (serum K+) levels leads to the reoccurrence of symptoms and rehospitalization of the patient. In the second proposed management scenario, interdisciplinary team discussions around differing tolerances and approaches to raised serum K+ levels lead to maintenance of guideline-directed RAASi doses with the help of close monitoring of the patient, introduction of a low potassium diet, and prescription of potassium binder therapy.
Conclusion: Collaborative multispecialty team management of HF patients may enable successful management of hyperkalemia without the need for discontinuation of guideline-directed RAASi therapy. Collaboration could extend to regular virtual or face-to-face cardiorenal clinics, where complex cases can be discussed, and local guidelines and processes can be developed.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


