Adam A Saleh, Rajdeepsingh Waghela, Shayan Amini, Joshua Moskow, Malcom Irani, Christopher Fan, Kerri Glassner, Bincy P Abraham
{"title":"A Guide to De-escalation of Combination Therapy in Inflammatory Bowel Disease: A Retrospective Cohort Study.","authors":"Adam A Saleh, Rajdeepsingh Waghela, Shayan Amini, Joshua Moskow, Malcom Irani, Christopher Fan, Kerri Glassner, Bincy P Abraham","doi":"10.1093/crocol/otaf026","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Advanced combination therapy with biologics and small molecules has seen more widespread implementation for inflammatory bowel disease (IBD). However, there is a paucity of data available to guide the successful de-escalation of combination therapy following the achievement of disease remission. Therefore, we pursued this retrospective study to evaluate our center's approach to de-escalation of these patients.</p><p><strong>Methods: </strong>IBD patients undergoing de-escalation of combination biologic therapy from May 2017 to March 2023 with a follow-up visit were included. The need for re-escalation, steroid therapy, and hospitalization at follow-up was compared between the de-escalation method, adherence, patient demographics, disease characteristics, and measures of disease activity.</p><p><strong>Results: </strong>Fifty IBD patients underwent de-escalation, with a median age of 35.7 years. All 50 patients had a follow-up visit within a median of 168 (111) days. Patients were divided into two groups with 12 (24%) patients requiring re-escalation of therapy and 38 (76%) able to maintain or further de-escalate. Of those that required re-escalation, 3 (25%) required the use of systemic steroids and none required hospitalization for IBD. Non-adherence to the de-escalation plan significantly correlated with the need for re-escalation (<i>P</i> < .001).</p><p><strong>Conclusions: </strong>Patient adherence and the number of prior failed biologic therapies were identified as potential risk factors for re-escalation. The type of agent being de-escalated (biologic or Janus kinase inhibitors [JAKi] did not correlate with the need for re-escalation).</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"7 2","pages":"otaf026"},"PeriodicalIF":1.8000,"publicationDate":"2025-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12048838/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otaf026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Advanced combination therapy with biologics and small molecules has seen more widespread implementation for inflammatory bowel disease (IBD). However, there is a paucity of data available to guide the successful de-escalation of combination therapy following the achievement of disease remission. Therefore, we pursued this retrospective study to evaluate our center's approach to de-escalation of these patients.
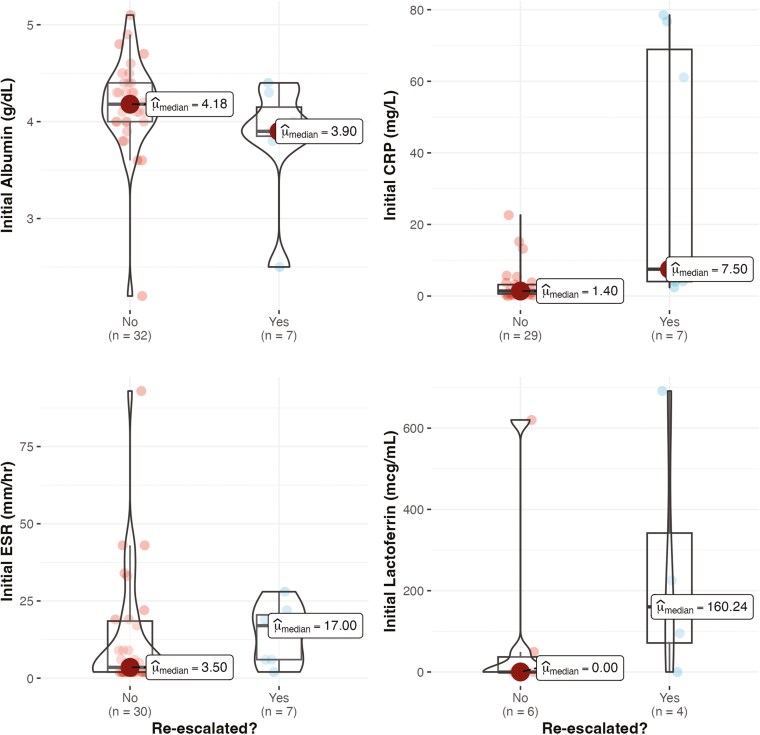
Methods: IBD patients undergoing de-escalation of combination biologic therapy from May 2017 to March 2023 with a follow-up visit were included. The need for re-escalation, steroid therapy, and hospitalization at follow-up was compared between the de-escalation method, adherence, patient demographics, disease characteristics, and measures of disease activity.
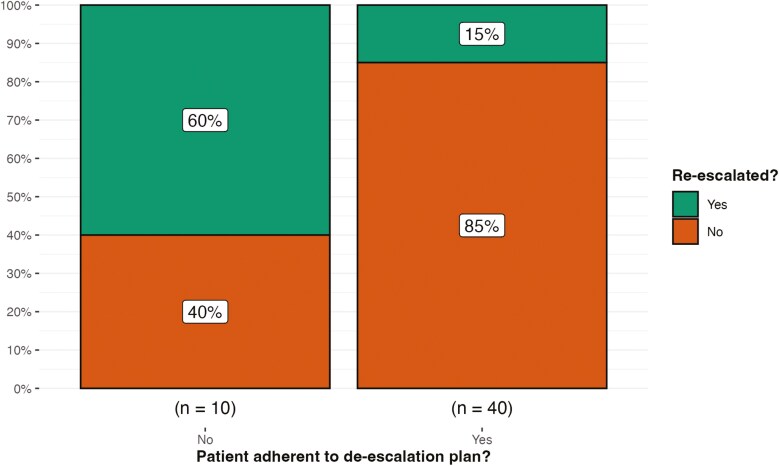
Results: Fifty IBD patients underwent de-escalation, with a median age of 35.7 years. All 50 patients had a follow-up visit within a median of 168 (111) days. Patients were divided into two groups with 12 (24%) patients requiring re-escalation of therapy and 38 (76%) able to maintain or further de-escalate. Of those that required re-escalation, 3 (25%) required the use of systemic steroids and none required hospitalization for IBD. Non-adherence to the de-escalation plan significantly correlated with the need for re-escalation (P < .001).
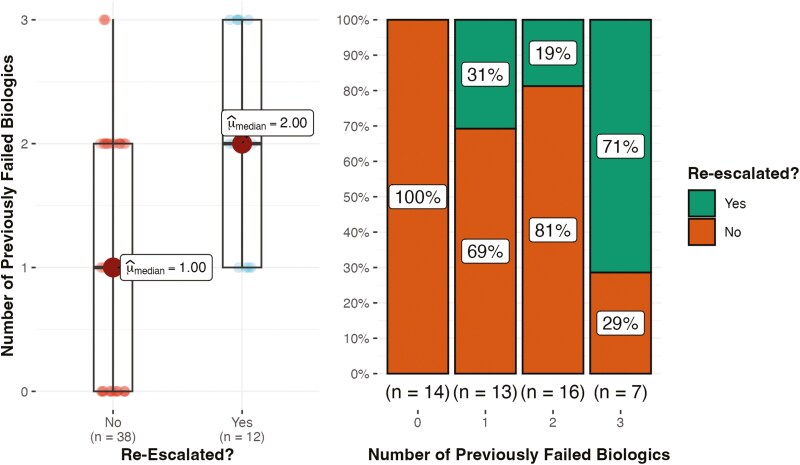
Conclusions: Patient adherence and the number of prior failed biologic therapies were identified as potential risk factors for re-escalation. The type of agent being de-escalated (biologic or Janus kinase inhibitors [JAKi] did not correlate with the need for re-escalation).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


