Zhiyuan Tan, Swantje Völler, Anyue Yin, Amy Rieborn, Hans Gelderblom, Tom van der Hulle, Catherijne A J Knibbe, Dirk Jan A R Moes
{"title":"Model-Informed Dose Optimization of Pazopanib in Real-World Patients with Cancer.","authors":"Zhiyuan Tan, Swantje Völler, Anyue Yin, Amy Rieborn, Hans Gelderblom, Tom van der Hulle, Catherijne A J Knibbe, Dirk Jan A R Moes","doi":"10.1007/s40262-025-01504-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Pazopanib is approved for metastatic renal cell carcinoma (mRCC) and soft tissue sarcoma (STS) in a dose of 800 mg once daily (QD) taken under fasted conditions. In clinical practice, approximately 60% of patients require dose reductions due to toxicity, with severe liver toxicity necessitating treatment interruptions in over 10% of cases. While a trough concentration (C<sub>min,ss</sub>) target of ≥ 20.5 mg/L has been established for mRCC efficacy, no specific threshold exists for liver toxicity. The objectives of this study were to develop a population pharmacokinetic (POPPK), an exposure-liver toxicity, and an exposure-tumor size dynamics model to optimize pazopanib initial dose in real-world patients.</p><p><strong>Methods: </strong>In total, 135 patients were included and treated with a median starting dose of 800 mg (interquartile range, IQR: 600-800 mg) QD pazopanib fasted with a median follow-up of 120 (IQR 63-372) days. A population pharmacokinetic model was developed using 460 concentration measurements from 135 patients. Exposure-liver toxicity was evaluated using time-to-event modeling, and exposure-tumor size dynamics was evaluated using tumor growth modelling.</p><p><strong>Results: </strong>The liver toxicity model, with 27 cases of grade ≥ 2 liver toxicity out of 135 patients (20%), identified a C<sub>min,ss</sub> threshold of > 34 mg/L associated with a 3.35-fold increased toxicity risk (P < 0.01). Model simulations showed that an initial dose of 600 mg QD significantly reduced liver toxicity risk (P < 0.001) while maintaining C<sub>min,ss</sub> ≥ 20.5 mg/L for 76% of the simulated individuals. Tumor size dynamics were analyzed using baseline and posttreatment tumor size measurements from 111 patients. The introduction of primary resistance by using a mixture model improved the model fit significantly. Tumor growth and decay rates differed between mRCC and STS but showed no pazopanib exposure dependency across the studied range, suggesting maximal tumor inhibition at current exposure levels.</p><p><strong>Conclusions: </strong>These findings suggest that an initial pazopanib dose of 600 mg fasted, followed by model-informed precision dosing to maintain C<sub>min,ss</sub> between 20 and 34 mg/L, may improve efficacy-toxicity balance and mitigate treatment interruptions.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":"64 5","pages":"715-728"},"PeriodicalIF":4.0000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12064635/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-025-01504-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/22 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: Pazopanib is approved for metastatic renal cell carcinoma (mRCC) and soft tissue sarcoma (STS) in a dose of 800 mg once daily (QD) taken under fasted conditions. In clinical practice, approximately 60% of patients require dose reductions due to toxicity, with severe liver toxicity necessitating treatment interruptions in over 10% of cases. While a trough concentration (Cmin,ss) target of ≥ 20.5 mg/L has been established for mRCC efficacy, no specific threshold exists for liver toxicity. The objectives of this study were to develop a population pharmacokinetic (POPPK), an exposure-liver toxicity, and an exposure-tumor size dynamics model to optimize pazopanib initial dose in real-world patients.
Methods: In total, 135 patients were included and treated with a median starting dose of 800 mg (interquartile range, IQR: 600-800 mg) QD pazopanib fasted with a median follow-up of 120 (IQR 63-372) days. A population pharmacokinetic model was developed using 460 concentration measurements from 135 patients. Exposure-liver toxicity was evaluated using time-to-event modeling, and exposure-tumor size dynamics was evaluated using tumor growth modelling.
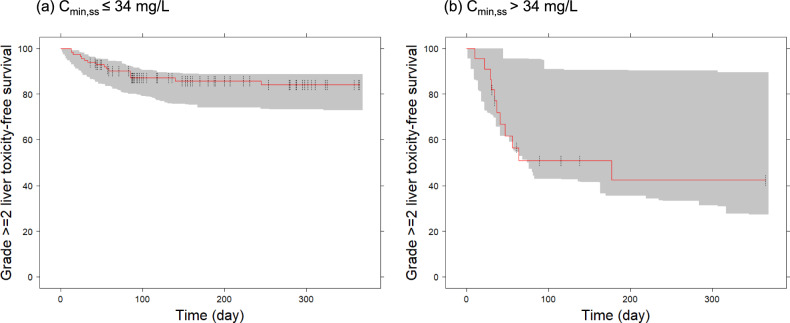
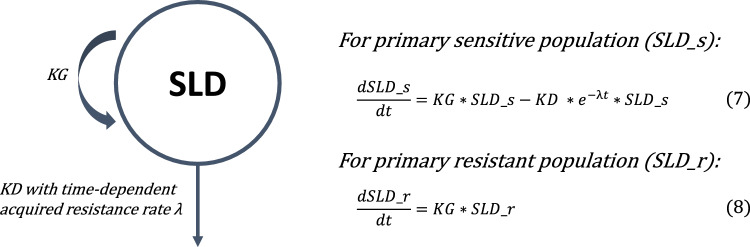
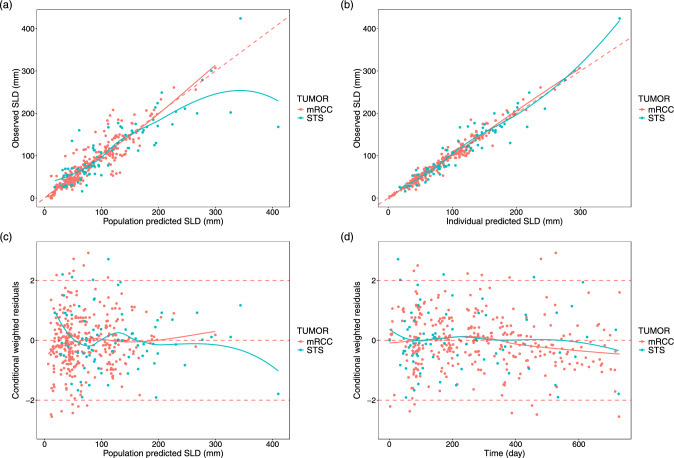
Results: The liver toxicity model, with 27 cases of grade ≥ 2 liver toxicity out of 135 patients (20%), identified a Cmin,ss threshold of > 34 mg/L associated with a 3.35-fold increased toxicity risk (P < 0.01). Model simulations showed that an initial dose of 600 mg QD significantly reduced liver toxicity risk (P < 0.001) while maintaining Cmin,ss ≥ 20.5 mg/L for 76% of the simulated individuals. Tumor size dynamics were analyzed using baseline and posttreatment tumor size measurements from 111 patients. The introduction of primary resistance by using a mixture model improved the model fit significantly. Tumor growth and decay rates differed between mRCC and STS but showed no pazopanib exposure dependency across the studied range, suggesting maximal tumor inhibition at current exposure levels.
Conclusions: These findings suggest that an initial pazopanib dose of 600 mg fasted, followed by model-informed precision dosing to maintain Cmin,ss between 20 and 34 mg/L, may improve efficacy-toxicity balance and mitigate treatment interruptions.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


