Jie Pan, Seungwon Lee, Cheligeer Cheligeer, Bing Li, Guosong Wu, Catherine A Eastwood, Yuan Xu, Hude Quan
{"title":"Assessing the validity of ICD-10 administrative data in coding comorbidities.","authors":"Jie Pan, Seungwon Lee, Cheligeer Cheligeer, Bing Li, Guosong Wu, Catherine A Eastwood, Yuan Xu, Hude Quan","doi":"10.1136/bmjhci-2024-101381","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Administrative data are commonly used to inform chronic disease prevalence and support health informatic research. This study assessed the validity of coding comorbidities in the International Classification of Diseases, 10th Revision (ICD-10) administrative data.</p><p><strong>Methods: </strong>We analysed three chart review cohorts (4008 patients in 2003, 3045 in 2015 and 9024 in 2022) in Alberta, Canada. Nurse reviewers assessed the presence of 17 clinical conditions using a consistent protocol. The reviews were linked with administrative data using unique patient identifiers. We compared the accuracy in coding comorbidity by ICD-10, using chart review data as the reference standard.</p><p><strong>Results: </strong>Our findings showed that the mean difference in prevalence between chart reviews and ICD-10 for these 17 conditions was 2.1% in 2003, 7.6% in 2015 and 6.3% in 2022. Some conditions were relatively stable, such as diabetes (1.9%, 2.1% and 1.1%) and metastatic cancer (0.3%, 1.1% and 0.4%). For these 17 conditions, the sensitivity ranged from 39.6-85.1% in 2003, 1.3%-85.2% in 2015 and 3.0-89.7% in 2022. The C-statistics for predicting in-hospital mortality using comorbidities by ICD-10 were 0.84 in 2003, 0.81 in 2015 and 0.78 in 2022.</p><p><strong>Discussion: </strong>The undercoding could be primarily due to the increase in hospital patient volumes and the limited time allocated to coding specialists. There is the potential to develop artificial intelligence methods based on electronic health records to support coding practices and improve data quality.</p><p><strong>Conclusion: </strong>Comorbidities were increasingly undercoded over 20 years. The validity of ICD-10 decreased but remained relatively stable for certain conditions mandated for coding. The undercoding exerted minimal impact on in-hospital mortality prediction.</p>","PeriodicalId":9050,"journal":{"name":"BMJ Health & Care Informatics","volume":"32 1","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12083369/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Health & Care Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjhci-2024-101381","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Administrative data are commonly used to inform chronic disease prevalence and support health informatic research. This study assessed the validity of coding comorbidities in the International Classification of Diseases, 10th Revision (ICD-10) administrative data.
Methods: We analysed three chart review cohorts (4008 patients in 2003, 3045 in 2015 and 9024 in 2022) in Alberta, Canada. Nurse reviewers assessed the presence of 17 clinical conditions using a consistent protocol. The reviews were linked with administrative data using unique patient identifiers. We compared the accuracy in coding comorbidity by ICD-10, using chart review data as the reference standard.
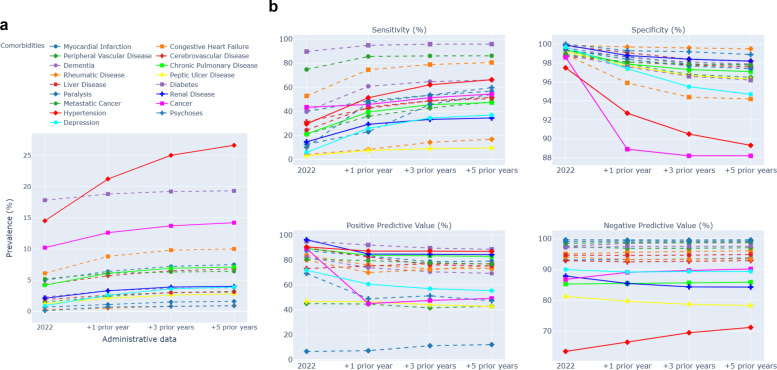
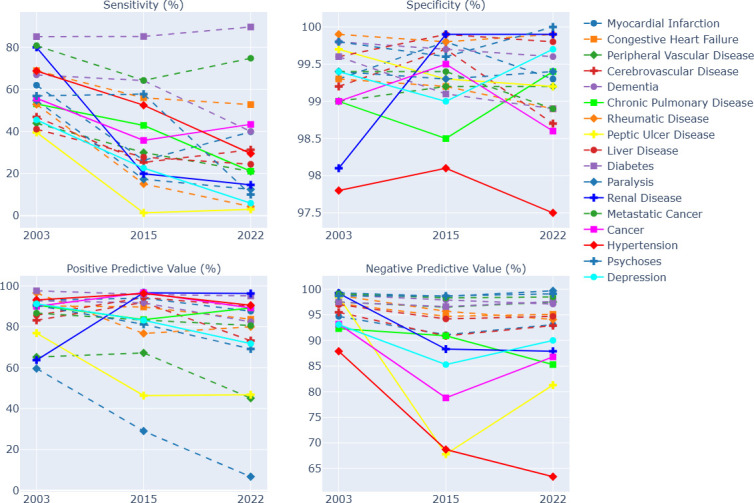
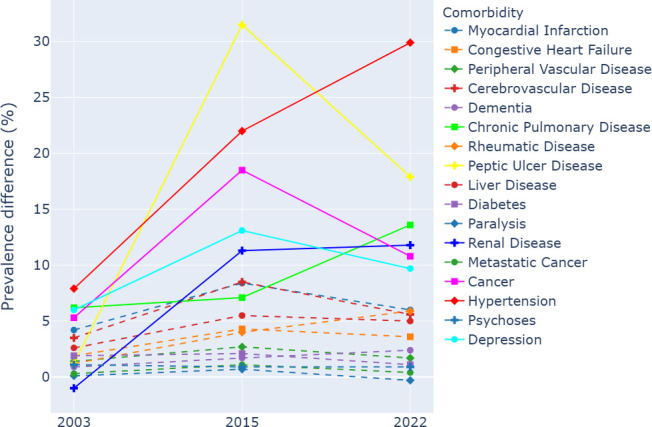
Results: Our findings showed that the mean difference in prevalence between chart reviews and ICD-10 for these 17 conditions was 2.1% in 2003, 7.6% in 2015 and 6.3% in 2022. Some conditions were relatively stable, such as diabetes (1.9%, 2.1% and 1.1%) and metastatic cancer (0.3%, 1.1% and 0.4%). For these 17 conditions, the sensitivity ranged from 39.6-85.1% in 2003, 1.3%-85.2% in 2015 and 3.0-89.7% in 2022. The C-statistics for predicting in-hospital mortality using comorbidities by ICD-10 were 0.84 in 2003, 0.81 in 2015 and 0.78 in 2022.
Discussion: The undercoding could be primarily due to the increase in hospital patient volumes and the limited time allocated to coding specialists. There is the potential to develop artificial intelligence methods based on electronic health records to support coding practices and improve data quality.
Conclusion: Comorbidities were increasingly undercoded over 20 years. The validity of ICD-10 decreased but remained relatively stable for certain conditions mandated for coding. The undercoding exerted minimal impact on in-hospital mortality prediction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


