Sophia D Sakka, Danai Georgakopoulou, Artemis Doulgeraki, Andreas H Krieg, John Anastasopoulos, Gabor Szinnai, Christina Kanaka-Gantenbein
{"title":"Burosumab treatment of a child with McCune-Albright syndrome/polyostotic fibrous dysplasia: challenges and benefits.","authors":"Sophia D Sakka, Danai Georgakopoulou, Artemis Doulgeraki, Andreas H Krieg, John Anastasopoulos, Gabor Szinnai, Christina Kanaka-Gantenbein","doi":"10.1093/jbmrpl/ziaf042","DOIUrl":null,"url":null,"abstract":"<p><p>Fibrous dysplasia/McCune-Albright syndrome (FD/MAS) is a rare condition caused by a mutation in the GNAS locus. Apart from endocrinopathies, some cases are characterized by excessive fibroblast growth factor 23 (FGF23) production from abnormal fibro-osseous tissue in FD lesions, resulting in increased renal phosphate excretion. We present a girl with FD/MAS and severe skeletal burden, evidenced by the presence of polyostotic fibrous dysplasia, which was complicated with bone fractures. She also had hyperthyroidism and GnRH-independent precocious puberty. She received zoledronic acid infusions in preparation for hip surgery. Despite optimal conventional management with oral phosphate and alphacalcidol, which was poorly tolerated, she presented persistent hypophosphatemia. To control hypophosphatemia and its deleterious effects on bone health, treatment with burosumab off-label at a dose of 0.66 mg/kg (20 mg) every 2 wk was initiated. Serum phosphate levels normalized within 2 wk of treatment. Laboratory results showed improvement in serum alkaline phosphatase (ALP) and PTH levels. After the second injection of burosumab, phosphate and PTH rose above the normal range with normal vitamin D levels; therefore, the interval between doses was increased to 3 wk, and calcium 500 mg daily was added. However, phosphate levels dropped again below normal range, so she had to return to 2-weekly injections of 20 mg. After 11 mo on burosumab, she remains with high normal phosphate levels and normal PTH and ALP values. Burosumab is well tolerated, with no adverse events to date. Burosumab is a human monoclonal antibody against FGF23 that reduces the risk of developing FGF23-mediated hypophosphatemia and its associated complications. Burosumab should be considered as an effective and safe alternative strategy for FGF23-mediated hypophosphatemia in FD/MAS for those who either cannot tolerate or do not respond to conventional therapy. To our knowledge, this is the fourth published case worldwide describing successful treatment with burosumab in FD/MAS.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"9 5","pages":"ziaf042"},"PeriodicalIF":2.4000,"publicationDate":"2025-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12035695/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziaf042","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
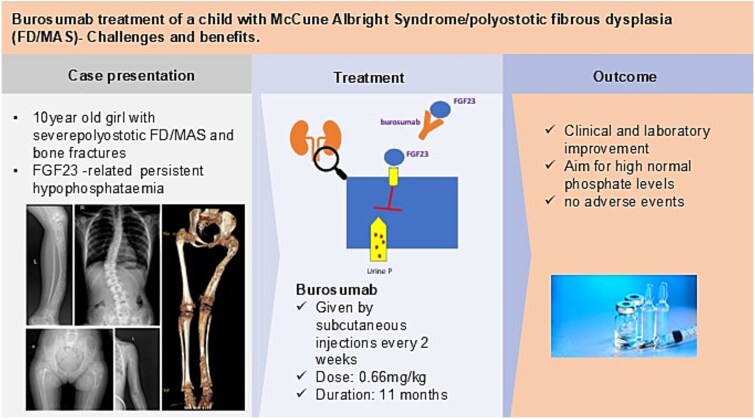
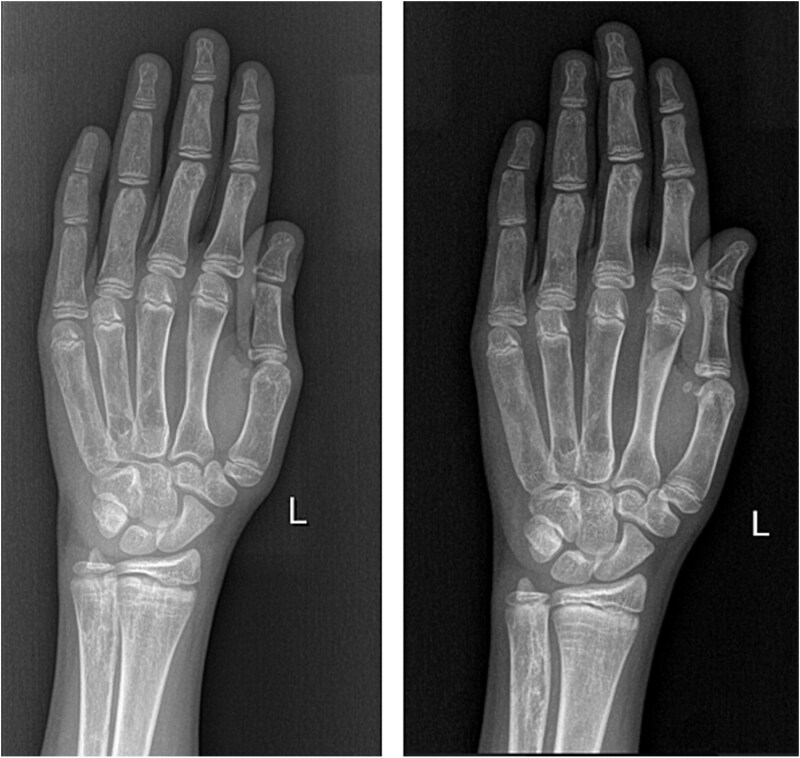
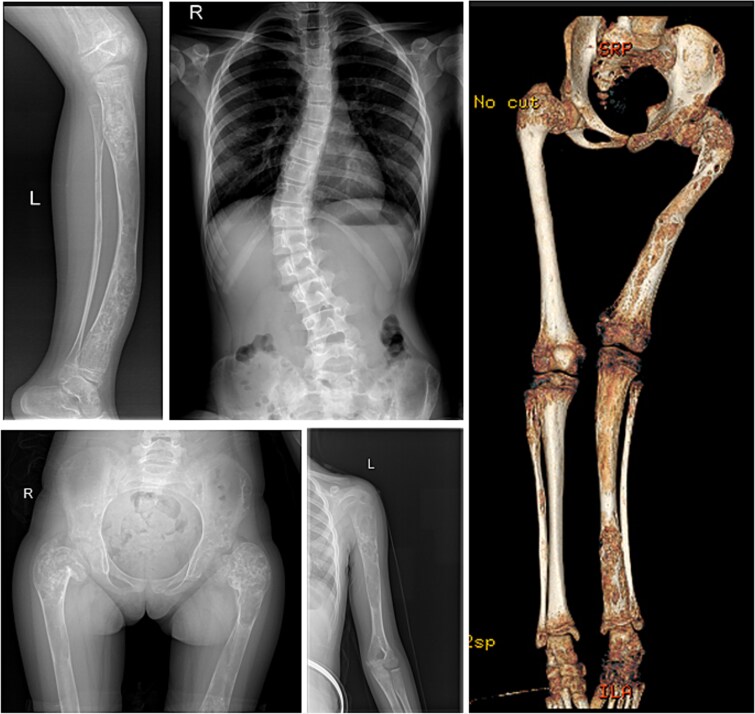
Fibrous dysplasia/McCune-Albright syndrome (FD/MAS) is a rare condition caused by a mutation in the GNAS locus. Apart from endocrinopathies, some cases are characterized by excessive fibroblast growth factor 23 (FGF23) production from abnormal fibro-osseous tissue in FD lesions, resulting in increased renal phosphate excretion. We present a girl with FD/MAS and severe skeletal burden, evidenced by the presence of polyostotic fibrous dysplasia, which was complicated with bone fractures. She also had hyperthyroidism and GnRH-independent precocious puberty. She received zoledronic acid infusions in preparation for hip surgery. Despite optimal conventional management with oral phosphate and alphacalcidol, which was poorly tolerated, she presented persistent hypophosphatemia. To control hypophosphatemia and its deleterious effects on bone health, treatment with burosumab off-label at a dose of 0.66 mg/kg (20 mg) every 2 wk was initiated. Serum phosphate levels normalized within 2 wk of treatment. Laboratory results showed improvement in serum alkaline phosphatase (ALP) and PTH levels. After the second injection of burosumab, phosphate and PTH rose above the normal range with normal vitamin D levels; therefore, the interval between doses was increased to 3 wk, and calcium 500 mg daily was added. However, phosphate levels dropped again below normal range, so she had to return to 2-weekly injections of 20 mg. After 11 mo on burosumab, she remains with high normal phosphate levels and normal PTH and ALP values. Burosumab is well tolerated, with no adverse events to date. Burosumab is a human monoclonal antibody against FGF23 that reduces the risk of developing FGF23-mediated hypophosphatemia and its associated complications. Burosumab should be considered as an effective and safe alternative strategy for FGF23-mediated hypophosphatemia in FD/MAS for those who either cannot tolerate or do not respond to conventional therapy. To our knowledge, this is the fourth published case worldwide describing successful treatment with burosumab in FD/MAS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


