Effect of host-protein test (TRAIL/IP-10/CRP) on antibiotic prescription and emergency department or urgent care center return visits: The JUNO pilot randomized controlled trial.
Adam J Singer, Judd E Hollander, Efrat R Kean, Hope Ring, W Frank Peacock, Karina M Soto-Ruiz, Sergey Motov, Joby Thoppil, Phyllis Hendry, Salim Halabi, Andrew C Meltzer, Gary F Headden, Tal Brosh-Nissimov, David Zeltser, Chad M Cannon
{"title":"Effect of host-protein test (TRAIL/IP-10/CRP) on antibiotic prescription and emergency department or urgent care center return visits: The JUNO pilot randomized controlled trial.","authors":"Adam J Singer, Judd E Hollander, Efrat R Kean, Hope Ring, W Frank Peacock, Karina M Soto-Ruiz, Sergey Motov, Joby Thoppil, Phyllis Hendry, Salim Halabi, Andrew C Meltzer, Gary F Headden, Tal Brosh-Nissimov, David Zeltser, Chad M Cannon","doi":"10.1111/acem.70031","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Determining etiology for adults with symptoms of lower respiratory tract infection (LRTI) is challenging. MeMed BV (MMBV), an FDA-cleared blood test, computationally integrates the levels of three host proteins to differentiate bacterial and viral infections. We evaluated MMBV's impact on safe antibiotic prescribing at emergency department/urgent care centers (ED/UC).</p><p><strong>Methods: </strong>The JUNO randomized controlled trial (RCT; NCT05762302) was a prespecified pilot phase of the JUPITER RCT. JUNO enrolled adult ED/UC patients with LRTI symptoms and clinician's consideration for antibiotic treatment. Inclusion criteria were fever within 7 days and one of cough, sputum production, dyspnea, or auscultation abnormality. Exclusion criteria were prior antibiotic use or immunosuppression. Patients were randomized to standard care (SC) or SC plus MMBV arms. JUNO's primary objective was to assess antibiotic prescription rate in the SC arm; the secondary objective was to assess JUPITER's study design.</p><p><strong>Results: </strong>Eleven centers randomized 260 patients, with 214 included (106 SC, 108 MMBV). Median (IQR) age was 40 (28-55.8) years, 57% were female, and 78.5% were enrolled at ED. Common symptoms were cough (93.0%) and chills (70.0%). Overall, antibiotic prescription rates were 30% (95% CI 22% to 40%) and 24% (95% CI 17% to 33%) in the SC arm versus the MMBV (absolute difference of -6% [95% CI -18% to 6%]). More antibiotics were given with bacterial MMBV scores (41% vs. 78%, absolute difference 37%, 95% CI 6% to 61%; n = 40) and less with viral MMBV scores (25% vs. 12%, absolute difference -13%, 95% CI -25% to 0%; n = 144) in the SC versus MMBV arms. There was no increase in ED/UC return visits (8% vs. 3%, difference -6%, 95% CI -12% to 1%) or hospitalizations (3% vs. 0%, difference -3%, 95% CI -7% to 1%) in the SC arm versus the MMBV arm.</p><p><strong>Conclusions: </strong>JUNO demonstrated that JUPITER's design results in 30% antibiotic prescription rate in the SC arm. JUNO supports that MMBV optimizes antibiotic prescriptions without increasing return ED/UC visits or hospitalizations.</p>","PeriodicalId":7105,"journal":{"name":"Academic Emergency Medicine","volume":" ","pages":"975-984"},"PeriodicalIF":3.2000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435126/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Academic Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/acem.70031","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/18 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
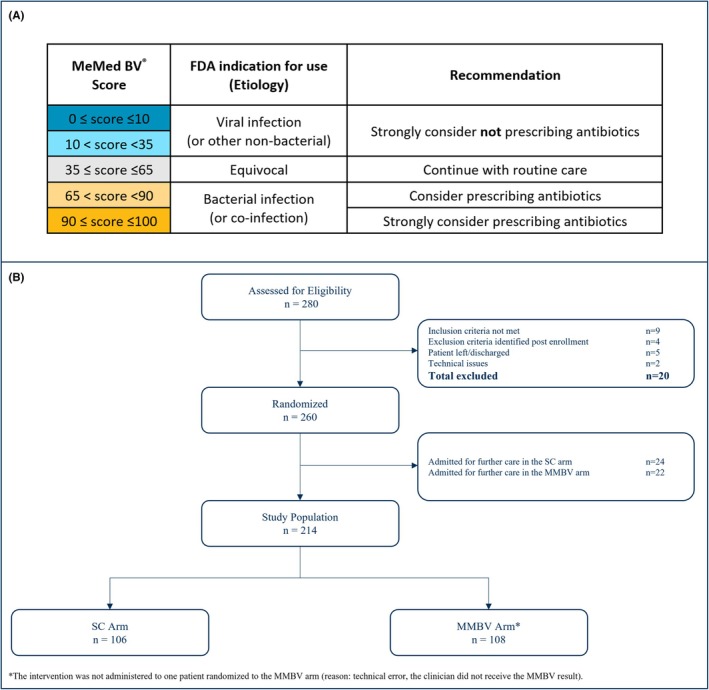
Objectives: Determining etiology for adults with symptoms of lower respiratory tract infection (LRTI) is challenging. MeMed BV (MMBV), an FDA-cleared blood test, computationally integrates the levels of three host proteins to differentiate bacterial and viral infections. We evaluated MMBV's impact on safe antibiotic prescribing at emergency department/urgent care centers (ED/UC).
Methods: The JUNO randomized controlled trial (RCT; NCT05762302) was a prespecified pilot phase of the JUPITER RCT. JUNO enrolled adult ED/UC patients with LRTI symptoms and clinician's consideration for antibiotic treatment. Inclusion criteria were fever within 7 days and one of cough, sputum production, dyspnea, or auscultation abnormality. Exclusion criteria were prior antibiotic use or immunosuppression. Patients were randomized to standard care (SC) or SC plus MMBV arms. JUNO's primary objective was to assess antibiotic prescription rate in the SC arm; the secondary objective was to assess JUPITER's study design.
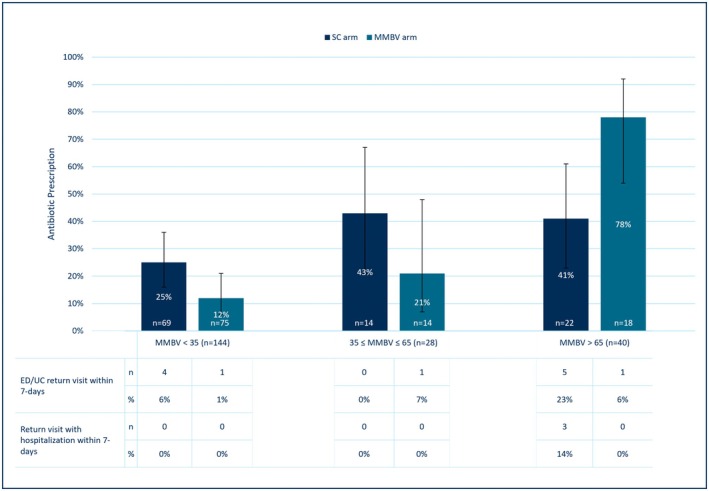
Results: Eleven centers randomized 260 patients, with 214 included (106 SC, 108 MMBV). Median (IQR) age was 40 (28-55.8) years, 57% were female, and 78.5% were enrolled at ED. Common symptoms were cough (93.0%) and chills (70.0%). Overall, antibiotic prescription rates were 30% (95% CI 22% to 40%) and 24% (95% CI 17% to 33%) in the SC arm versus the MMBV (absolute difference of -6% [95% CI -18% to 6%]). More antibiotics were given with bacterial MMBV scores (41% vs. 78%, absolute difference 37%, 95% CI 6% to 61%; n = 40) and less with viral MMBV scores (25% vs. 12%, absolute difference -13%, 95% CI -25% to 0%; n = 144) in the SC versus MMBV arms. There was no increase in ED/UC return visits (8% vs. 3%, difference -6%, 95% CI -12% to 1%) or hospitalizations (3% vs. 0%, difference -3%, 95% CI -7% to 1%) in the SC arm versus the MMBV arm.
Conclusions: JUNO demonstrated that JUPITER's design results in 30% antibiotic prescription rate in the SC arm. JUNO supports that MMBV optimizes antibiotic prescriptions without increasing return ED/UC visits or hospitalizations.
目的:确定成人下呼吸道感染(LRTI)症状的病因是具有挑战性的。MeMed BV (MMBV)是一种获得fda批准的血液测试,通过计算整合三种宿主蛋白的水平来区分细菌和病毒感染。我们评估了MMBV对急诊科/紧急护理中心(ED/UC)安全抗生素处方的影响。方法:JUNO随机对照试验(RCT;NCT05762302)是JUPITER RCT预先指定的试点阶段。JUNO纳入了有下呼吸道感染症状和临床医生考虑抗生素治疗的成人ED/UC患者。纳入标准为7天内发热,咳嗽、咳痰、呼吸困难或听诊异常之一。排除标准为既往使用抗生素或免疫抑制。患者被随机分为标准治疗组(SC)或SC + MMBV组。JUNO的主要目的是评估SC组的抗生素处方率;第二个目标是评估木星的研究设计。结果:11个中心随机分配260例患者,其中214例(106例SC, 108例MMBV)。中位(IQR)年龄为40(28-55.8)岁,57%为女性,78.5%在急诊科登记。常见症状为咳嗽(93.0%)和发冷(70.0%)。总体而言,与MMBV组相比,SC组的抗生素处方率分别为30% (95% CI 22%至40%)和24% (95% CI 17%至33%)(绝对差异为-6% [95% CI -18%至6%])。细菌性MMBV评分患者使用较多抗生素(41% vs. 78%,绝对差异37%,95% CI 6% ~ 61%;n = 40),而病毒MMBV评分更低(25% vs. 12%,绝对差-13%,95% CI -25% ~ 0%;n = 144), SC组与MMBV组比较。与MMBV组相比,SC组ED/UC的回访率(8%对3%,差异为-6%,95% CI为-12%至1%)或住院率(3%对0%,差异为-3%,95% CI为-7%至1%)均未增加。结论:JUNO证明JUPITER的设计使SC组的抗生素处方率达到30%。JUNO支持MMBV在不增加急诊/UC回访或住院的情况下优化抗生素处方。
期刊介绍:
Academic Emergency Medicine (AEM) is the official monthly publication of the Society for Academic Emergency Medicine (SAEM) and publishes information relevant to the practice, educational advancements, and investigation of emergency medicine. It is the second-largest peer-reviewed scientific journal in the specialty of emergency medicine.
The goal of AEM is to advance the science, education, and clinical practice of emergency medicine, to serve as a voice for the academic emergency medicine community, and to promote SAEM''s goals and objectives. Members and non-members worldwide depend on this journal for translational medicine relevant to emergency medicine, as well as for clinical news, case studies and more.
Each issue contains information relevant to the research, educational advancements, and practice in emergency medicine. Subject matter is diverse, including preclinical studies, clinical topics, health policy, and educational methods. The research of SAEM members contributes significantly to the scientific content and development of the journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


