Comparison of surgical outcomes between unilateral biportal endoscopic technique and open microdiscectomy in patients with single-level lumbar disc herniation: a single-center retrospective study in China.
Tianyao Ke, Qiulin He, Qiying Wang, Long Li, Changgui Shi, Jiaxue Zeng, Qing Li
{"title":"Comparison of surgical outcomes between unilateral biportal endoscopic technique and open microdiscectomy in patients with single-level lumbar disc herniation: a single-center retrospective study in China.","authors":"Tianyao Ke, Qiulin He, Qiying Wang, Long Li, Changgui Shi, Jiaxue Zeng, Qing Li","doi":"10.31616/asj.2024.0002","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>Single-center retrospective cohort analysis.</p><p><strong>Purpose: </strong>To compare surgical outcomes between the unilateral biportal endoscopic (UBE) and open microdiscectomy for the treatment of single-level lumbar disc herniation (LDH).</p><p><strong>Overview of literature: </strong>Open microdiscectomy remains the gold standard for LDH, while UBE has emerged as a minimally invasive alternative. However, comparative evidence on efficacy, safety, and recovery profiles remains limited.</p><p><strong>Methods: </strong>This was a single-center retrospective analysis of 46 patients with single-level LDH who underwent either the UBE surgery (n=22) or open microdiscectomy (n=24) between January 2020 and December 2022. Demographic information, perioperative data, and radiographic measurements were reviewed. Pain intensity, patient satisfaction, and quality of life were assessed using the Visual Analog Scale (VAS) and the Oswestry Disability Index (ODI) at 1-week, 3-month, and 12-month follow-ups.</p><p><strong>Results: </strong>The mean operative time in the UBE group (86.1±11.4 minutes) was significantly longer than in the open microdiscectomy group (72.3±8.0 minutes, p=0.032). UBE was associated with significantly lower estimated blood loss (54.1±13.7 mL vs. 92.5±11.6 mL, p=0.001) and shorter hospital stay (3.7±1.2 days vs. 6.6±1.4 days, p=0.001). The mean VAS score for back pain at 1 week was significantly better in the UBE group (1.88±0.60 vs. 3.59±0.72, p=0.004). However, both surgical techniques showed similar long-term results regarding disc height, disc angle changes, and patient-reported outcomes.</p><p><strong>Conclusions: </strong>Despite the longer operative time, UBE is associated with reduced estimated blood loss and shorter hospital stays, offering a minimally invasive alternative with early postoperative pain relief. Conversely, open microdiscectomy, the conventional treatment approach, demonstrates comparable efficacy in long-term clinical outcomes despite its more invasive nature. Both methods show similar rates of complications and recurrent disc herniation. UBE is a viable alternative to open microdiscectomy, depending on individual patient considerations and surgical preferences.</p>","PeriodicalId":8555,"journal":{"name":"Asian Spine Journal","volume":" ","pages":"600-608"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400092/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Spine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31616/asj.2024.0002","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/11 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: Single-center retrospective cohort analysis.
Purpose: To compare surgical outcomes between the unilateral biportal endoscopic (UBE) and open microdiscectomy for the treatment of single-level lumbar disc herniation (LDH).
Overview of literature: Open microdiscectomy remains the gold standard for LDH, while UBE has emerged as a minimally invasive alternative. However, comparative evidence on efficacy, safety, and recovery profiles remains limited.
Methods: This was a single-center retrospective analysis of 46 patients with single-level LDH who underwent either the UBE surgery (n=22) or open microdiscectomy (n=24) between January 2020 and December 2022. Demographic information, perioperative data, and radiographic measurements were reviewed. Pain intensity, patient satisfaction, and quality of life were assessed using the Visual Analog Scale (VAS) and the Oswestry Disability Index (ODI) at 1-week, 3-month, and 12-month follow-ups.
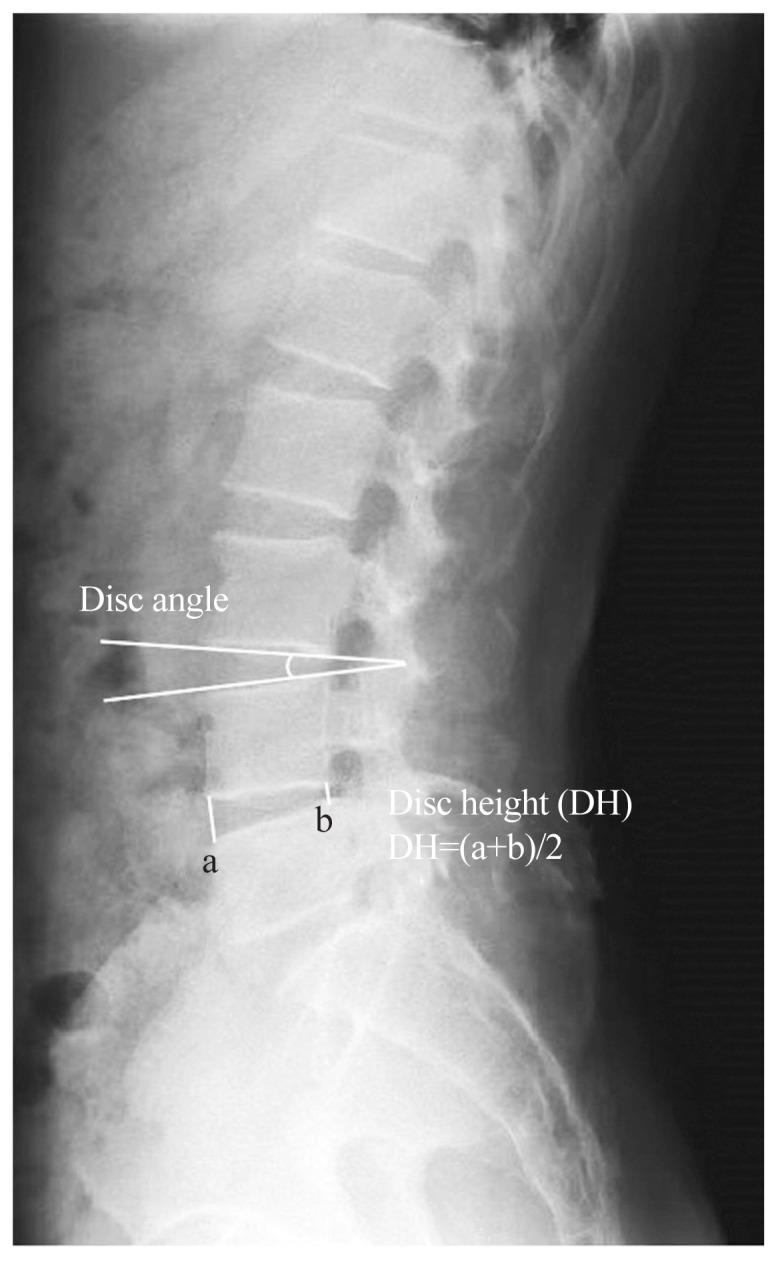
Results: The mean operative time in the UBE group (86.1±11.4 minutes) was significantly longer than in the open microdiscectomy group (72.3±8.0 minutes, p=0.032). UBE was associated with significantly lower estimated blood loss (54.1±13.7 mL vs. 92.5±11.6 mL, p=0.001) and shorter hospital stay (3.7±1.2 days vs. 6.6±1.4 days, p=0.001). The mean VAS score for back pain at 1 week was significantly better in the UBE group (1.88±0.60 vs. 3.59±0.72, p=0.004). However, both surgical techniques showed similar long-term results regarding disc height, disc angle changes, and patient-reported outcomes.
Conclusions: Despite the longer operative time, UBE is associated with reduced estimated blood loss and shorter hospital stays, offering a minimally invasive alternative with early postoperative pain relief. Conversely, open microdiscectomy, the conventional treatment approach, demonstrates comparable efficacy in long-term clinical outcomes despite its more invasive nature. Both methods show similar rates of complications and recurrent disc herniation. UBE is a viable alternative to open microdiscectomy, depending on individual patient considerations and surgical preferences.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


