Kate Honeyford, Alf Timney, Runa Lazzarino, John Welch, Andrew Jonathan Brent, Anne Kinderlerer, Peter Ghazal, Anthony C Gordon, Shashank Patil, Graham Cooke, Ceire E Costelloe
{"title":"Digital innovation in healthcare: quantifying the impact of digital sepsis screening tools on patient outcomes-a multi-site natural experiment.","authors":"Kate Honeyford, Alf Timney, Runa Lazzarino, John Welch, Andrew Jonathan Brent, Anne Kinderlerer, Peter Ghazal, Anthony C Gordon, Shashank Patil, Graham Cooke, Ceire E Costelloe","doi":"10.1136/bmjhci-2024-101141","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The National Health Service (NHS) 'move to digital' incorporating electronic patient record systems (EPR) facilitates the translation of paper-based screening tools into digital systems, including digital sepsis alerts. We evaluated the impact of sepsis screening tools on in-patient 30-day mortality across four multi-hospital NHS Trusts, each using a different algorithm for early detection of sepsis.</p><p><strong>Methods: </strong>Using quasi-experimental methods, we investigated the impact of the screening tools. Individual-level EPR data for 718 000 patients between 2010 and 2020 were extracted to assess the impact on a target cohort and control cohort using interrupted time series analysis, based on a binomial regression model. We included one Trust which uses a paper-based screening tool to compare the impact of digital and paper-based interventions, and one Trust which did not introduce a sepsis screening tool, but did introduce an EPR.</p><p><strong>Results: </strong>All Trusts had lower odds of mortality, between 5% and 12%, after the introduction of the sepsis screening tool, before adjustment for pre-existing trends or patient casemix. After adjustment for existing trends, there was a significant reduction in mortality in two of the three Trusts which introduced sepsis screening tools. We also observed age-specific effects across Trusts.</p><p><strong>Conclusion: </strong>Our findings confirm that patients with similar profiles have a lower mortality risk, consistent with our previous work. This study, conducted across multiple NHS Trusts, suggests that alerts could be tailored to specific patient groups based on age-related effects. Different Trusts may require unique indicators, thresholds, actions and treatments. Including additional EPR information could further enhance personalised care.</p>","PeriodicalId":9050,"journal":{"name":"BMJ Health & Care Informatics","volume":"32 1","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-04-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12035476/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Health & Care Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjhci-2024-101141","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The National Health Service (NHS) 'move to digital' incorporating electronic patient record systems (EPR) facilitates the translation of paper-based screening tools into digital systems, including digital sepsis alerts. We evaluated the impact of sepsis screening tools on in-patient 30-day mortality across four multi-hospital NHS Trusts, each using a different algorithm for early detection of sepsis.
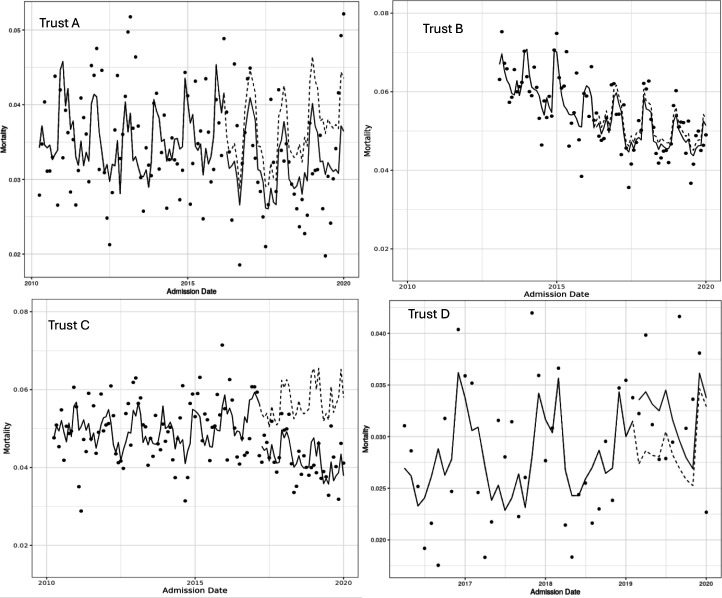
Methods: Using quasi-experimental methods, we investigated the impact of the screening tools. Individual-level EPR data for 718 000 patients between 2010 and 2020 were extracted to assess the impact on a target cohort and control cohort using interrupted time series analysis, based on a binomial regression model. We included one Trust which uses a paper-based screening tool to compare the impact of digital and paper-based interventions, and one Trust which did not introduce a sepsis screening tool, but did introduce an EPR.
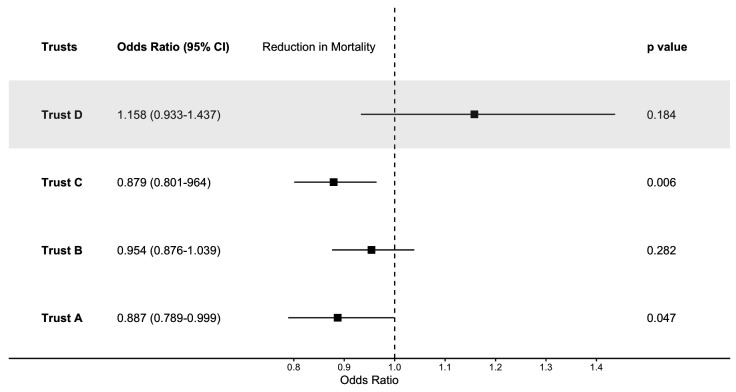
Results: All Trusts had lower odds of mortality, between 5% and 12%, after the introduction of the sepsis screening tool, before adjustment for pre-existing trends or patient casemix. After adjustment for existing trends, there was a significant reduction in mortality in two of the three Trusts which introduced sepsis screening tools. We also observed age-specific effects across Trusts.
Conclusion: Our findings confirm that patients with similar profiles have a lower mortality risk, consistent with our previous work. This study, conducted across multiple NHS Trusts, suggests that alerts could be tailored to specific patient groups based on age-related effects. Different Trusts may require unique indicators, thresholds, actions and treatments. Including additional EPR information could further enhance personalised care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


