{"title":"The Phenotypes of Asthma-Bronchiectasis Overlap: Clinical Characteristics and Outcomes.","authors":"Zhen-Hong Lin, Cui-Xia Pan, Jia-Hui He, Xiao-Xian Zhang, Sheng-Zhu Lin, Qing-Ling Zhang, Mei Dai, Wei-Quan Liang, Wei-Jie Guan","doi":"10.4168/aair.2025.17.2.196","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Asthma-bronchiectasis overlap (ABO) encompasses heterogeneous manifestations, which may predict distinct clinical outcomes. We sought to identify the clinical phenotypes of ABO and compare them to asthma alone or bronchiectasis alone.</p><p><strong>Methods: </strong>In this retrospective cohort study, we extracted electronic medical records from 292 inpatients with ABO, 901 inpatients with asthma alone, and 1,192 inpatients with bronchiectasis alone who were hospitalized between 2015 and 2020. We phenotyped ABO using 2-step unsupervised clustering analysis by using an independent cohort (n = 76).</p><p><strong>Results: </strong>Compared to asthma or bronchiectasis alone, ABO exhibited greater disease severity and worse clinical outcomes. We identified 3 ABO phenotypes: asthma-dominant ABO (ABO-A, n = 100) with more prominent asthma symptoms; bronchiectasis-dominant ABO (ABO-B, n = 89) with more pronounced features of bronchiectasis; and co-existence of asthma and severe bronchiectasis (ABO-S, n = 103) with worse clinical outcomes. Compared to ABO-B, both ABO-A and ABO-S were associated with significantly higher blood neutrophil ratios (55.8% vs. 59.1% vs. 64.4%, <i>P</i> < 0.001), poorer lung function (FEV1% predicted: 79.1% vs. 67.5% vs. 50.1%, <i>P</i> < 0.001), longer hospital stay (6.0 vs. 7.0 vs. 7.0 days, <i>P</i> = 0.004), and higher risks of hospitalization within the next 2 years (ABO-A: hazards ratio [HR], 3.76, 95% confidence interval [CI], 1.12-12.62, <i>P</i> = 0.032; ABO-S: HR, 4.05, 95% CI, 1.14-14.36, <i>P</i> = 0.031).</p><p><strong>Conclusions: </strong>The radiologic severity of bronchiectasis and the use of systemic corticosteroids can identify the clinical phenotypes of ABO. The heterogeneity of clinical manifestations may help formulate personalized management strategies and predict the prognosis of ABO.</p>","PeriodicalId":7547,"journal":{"name":"Allergy, Asthma & Immunology Research","volume":"17 2","pages":"196-211"},"PeriodicalIF":4.3000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11982639/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy, Asthma & Immunology Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4168/aair.2025.17.2.196","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Asthma-bronchiectasis overlap (ABO) encompasses heterogeneous manifestations, which may predict distinct clinical outcomes. We sought to identify the clinical phenotypes of ABO and compare them to asthma alone or bronchiectasis alone.
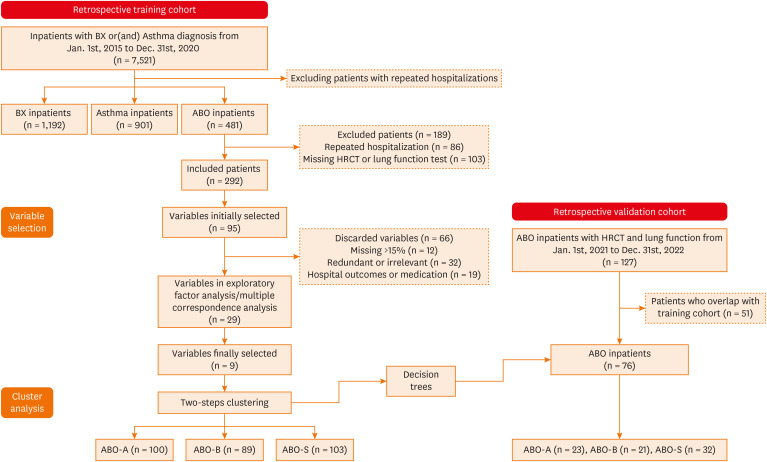
Methods: In this retrospective cohort study, we extracted electronic medical records from 292 inpatients with ABO, 901 inpatients with asthma alone, and 1,192 inpatients with bronchiectasis alone who were hospitalized between 2015 and 2020. We phenotyped ABO using 2-step unsupervised clustering analysis by using an independent cohort (n = 76).
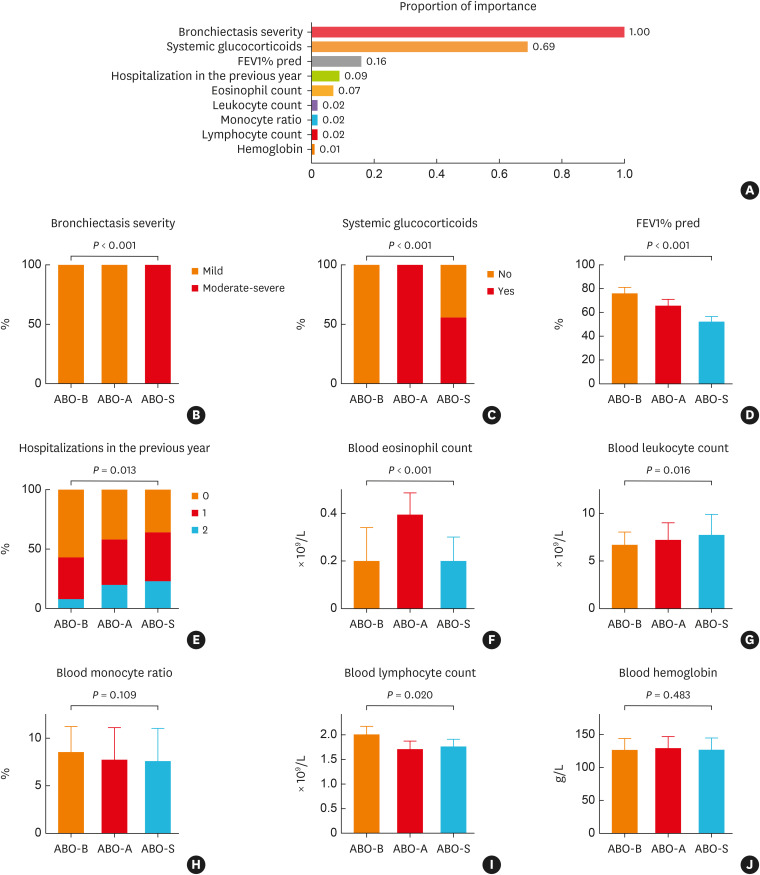
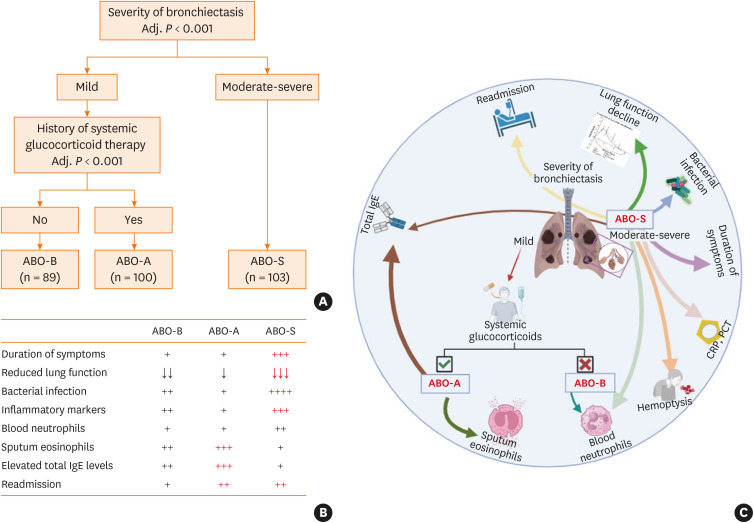
Results: Compared to asthma or bronchiectasis alone, ABO exhibited greater disease severity and worse clinical outcomes. We identified 3 ABO phenotypes: asthma-dominant ABO (ABO-A, n = 100) with more prominent asthma symptoms; bronchiectasis-dominant ABO (ABO-B, n = 89) with more pronounced features of bronchiectasis; and co-existence of asthma and severe bronchiectasis (ABO-S, n = 103) with worse clinical outcomes. Compared to ABO-B, both ABO-A and ABO-S were associated with significantly higher blood neutrophil ratios (55.8% vs. 59.1% vs. 64.4%, P < 0.001), poorer lung function (FEV1% predicted: 79.1% vs. 67.5% vs. 50.1%, P < 0.001), longer hospital stay (6.0 vs. 7.0 vs. 7.0 days, P = 0.004), and higher risks of hospitalization within the next 2 years (ABO-A: hazards ratio [HR], 3.76, 95% confidence interval [CI], 1.12-12.62, P = 0.032; ABO-S: HR, 4.05, 95% CI, 1.14-14.36, P = 0.031).
Conclusions: The radiologic severity of bronchiectasis and the use of systemic corticosteroids can identify the clinical phenotypes of ABO. The heterogeneity of clinical manifestations may help formulate personalized management strategies and predict the prognosis of ABO.
期刊介绍:
The journal features cutting-edge original research, brief communications, and state-of-the-art reviews in the specialties of allergy, asthma, and immunology, including clinical and experimental studies and instructive case reports. Contemporary reviews summarize information on topics for researchers and physicians in the fields of allergy and immunology. As of January 2017, AAIR do not accept case reports. However, if it is a clinically important case, authors can submit it in the form of letter to the Editor. Editorials and letters to the Editor explore controversial issues and encourage further discussion among physicians dealing with allergy, immunology, pediatric respirology, and related medical fields. AAIR also features topics in practice and management and recent advances in equipment and techniques for clinicians concerned with clinical manifestations of allergies and pediatric respiratory diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


