A. Selvanathan, S. Nazir, K. van Wyk, E. Simpson, V. Holmes, R. Hutton, F. White, B. C. Schwahn
{"title":"Benefits of Integrated Social Care in the Management of Patients With Inborn Errors of Metabolism","authors":"A. Selvanathan, S. Nazir, K. van Wyk, E. Simpson, V. Holmes, R. Hutton, F. White, B. C. Schwahn","doi":"10.1002/jmd2.70023","DOIUrl":null,"url":null,"abstract":"<p>The current cornerstone of the management of many small-molecule inborn errors of metabolism (IEMs) is a combination of dietary therapy and medication, with evidence for improved clinical outcomes. However, the burden imposed on patients and families is substantial. Many families also have to manage this burden in conjunction with other medical, psychosocial, and financial stressors. Adherence to the recommended treatment can therefore be extremely challenging, sometimes leading to sustained derangement of biochemical parameters and/or clinical deterioration. The treating team needs to work with the family to determine an individualized optimal management strategy, with targets that can be pragmatically achieved. This paper focusses on the role of social care in assisting patients with a range of different small-molecule IEMs, as well as their families and the medical team. We provide six case vignettes that illustrate how social care involvement, in addition to enhanced psychosocial support from the clinical team, resulted in improved outcomes. This included assisting with adjustment to a new diagnosis, exploring and addressing barriers to treatment adherence, and provision of ‘early help’ community supports. In some instances where this was not sufficient and risk of harm to the child was considered significant, social care involvement facilitated graded escalation from a “child in need” approach to formal child protection measures. We identified challenges in engaging social workers external to the metabolic team. This included a need for greater education about the medical condition and the risks associated with undertreatment, lack of protected time for metabolic case management, and a lack of preventative involvement of social workers during the initial hospitalization (impacting on patient rapport). We advocate for the integration of social care within the metabolic team as part of a more holistic model of care.</p>","PeriodicalId":14930,"journal":{"name":"JIMD reports","volume":"66 3","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2025-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jmd2.70023","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JIMD reports","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jmd2.70023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Biochemistry, Genetics and Molecular Biology","Score":null,"Total":0}
引用次数: 0
Abstract
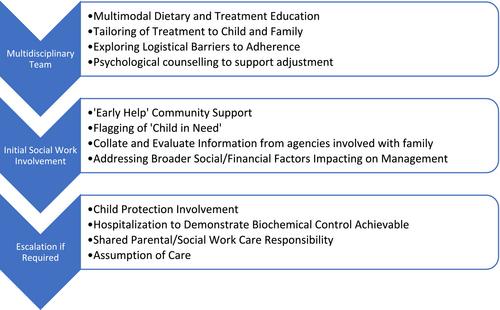
The current cornerstone of the management of many small-molecule inborn errors of metabolism (IEMs) is a combination of dietary therapy and medication, with evidence for improved clinical outcomes. However, the burden imposed on patients and families is substantial. Many families also have to manage this burden in conjunction with other medical, psychosocial, and financial stressors. Adherence to the recommended treatment can therefore be extremely challenging, sometimes leading to sustained derangement of biochemical parameters and/or clinical deterioration. The treating team needs to work with the family to determine an individualized optimal management strategy, with targets that can be pragmatically achieved. This paper focusses on the role of social care in assisting patients with a range of different small-molecule IEMs, as well as their families and the medical team. We provide six case vignettes that illustrate how social care involvement, in addition to enhanced psychosocial support from the clinical team, resulted in improved outcomes. This included assisting with adjustment to a new diagnosis, exploring and addressing barriers to treatment adherence, and provision of ‘early help’ community supports. In some instances where this was not sufficient and risk of harm to the child was considered significant, social care involvement facilitated graded escalation from a “child in need” approach to formal child protection measures. We identified challenges in engaging social workers external to the metabolic team. This included a need for greater education about the medical condition and the risks associated with undertreatment, lack of protected time for metabolic case management, and a lack of preventative involvement of social workers during the initial hospitalization (impacting on patient rapport). We advocate for the integration of social care within the metabolic team as part of a more holistic model of care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


