Ellie C Treloar, Jesse D Ey, Matheesha Herath, Nicholas P R Edwardes, Suzanne Edwards, Martin H Bruening, Guy J Maddern
{"title":"Optimizing ward rounds: systematic review and meta-analysis of interventions to enhance patient safety.","authors":"Ellie C Treloar, Jesse D Ey, Matheesha Herath, Nicholas P R Edwardes, Suzanne Edwards, Martin H Bruening, Guy J Maddern","doi":"10.1093/bjs/znaf041","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Poor quality ward rounds contribute to a large proportion of patient complications, delayed discharge, and increased hospital cost. This systematic review investigated all interventions aiming to improve patient and process-based outcomes in ward rounds.</p><p><strong>Methods: </strong>This systematic review was prospectively registered in PROSPERO, the international prospective register of systematic reviews (CRD42023394325). MEDLINE, Embase, Emcare, and PsycInfo were searched for studies with interventions aiming to improve ward round processes or patient outcomes in hospital settings. Studies were excluded if there was no baseline comparator or they were not in the ward round setting. Interventions were coded as checklist interventions (that is electronic or paper-based pro formas, templates, and checklists), structure interventions (that is defined rules or protocol to guide or standardize conduct), or other interventions. Outcomes were assessed via meta-analyses using the I2 statistic, Cochran's Q P value, and random-effects models. Risk of bias was assessed using the Cochrane Risk of Bias 2 tool for RCTs and the Newcastle-Ottawa scale for non-randomized studies.</p><p><strong>Results: </strong>This review included 84 studies, from 18 countries, in 23 specialties, involving 43 570 patients. Checklist interventions significantly reduced ICU length of stay, improved overall documentation, and did not increase ward round duration. Structure interventions did not increase the time spent per patient or impact 30-day readmission rates or patient length of stay.</p><p><strong>Conclusion: </strong>This is the first systematic review with meta-analyses synthesizing the evidence of all ward round interventions targeted at improving patient and process outcomes. Results from this review should be used to inform guidelines for the 'ideal ward round'.</p>","PeriodicalId":136,"journal":{"name":"British Journal of Surgery","volume":"112 4","pages":""},"PeriodicalIF":8.8000,"publicationDate":"2025-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11979594/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"British Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjs/znaf041","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Poor quality ward rounds contribute to a large proportion of patient complications, delayed discharge, and increased hospital cost. This systematic review investigated all interventions aiming to improve patient and process-based outcomes in ward rounds.
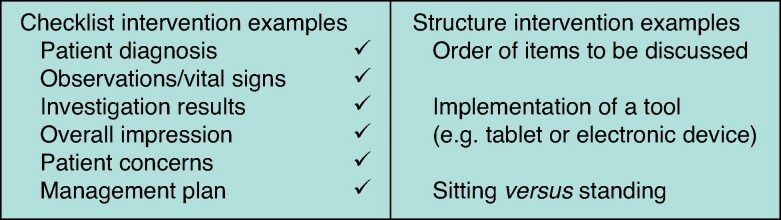
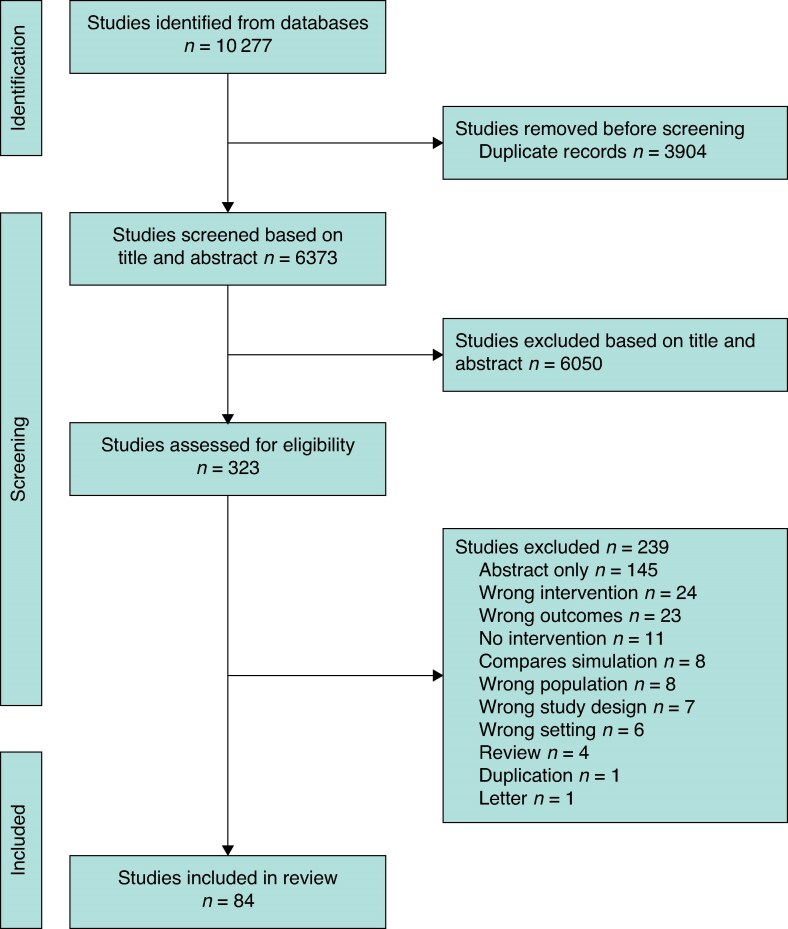
Methods: This systematic review was prospectively registered in PROSPERO, the international prospective register of systematic reviews (CRD42023394325). MEDLINE, Embase, Emcare, and PsycInfo were searched for studies with interventions aiming to improve ward round processes or patient outcomes in hospital settings. Studies were excluded if there was no baseline comparator or they were not in the ward round setting. Interventions were coded as checklist interventions (that is electronic or paper-based pro formas, templates, and checklists), structure interventions (that is defined rules or protocol to guide or standardize conduct), or other interventions. Outcomes were assessed via meta-analyses using the I2 statistic, Cochran's Q P value, and random-effects models. Risk of bias was assessed using the Cochrane Risk of Bias 2 tool for RCTs and the Newcastle-Ottawa scale for non-randomized studies.
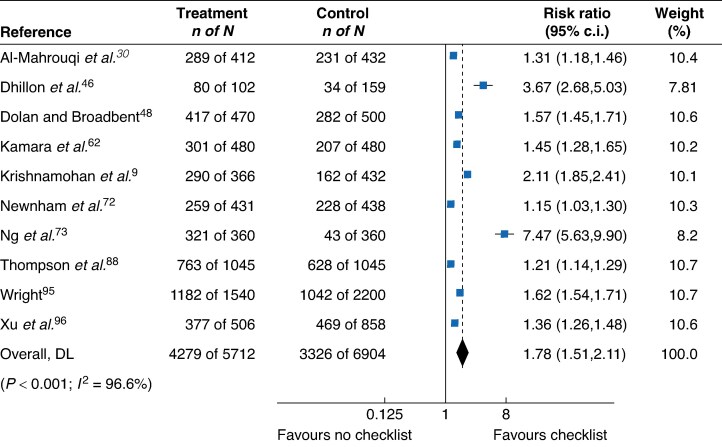
Results: This review included 84 studies, from 18 countries, in 23 specialties, involving 43 570 patients. Checklist interventions significantly reduced ICU length of stay, improved overall documentation, and did not increase ward round duration. Structure interventions did not increase the time spent per patient or impact 30-day readmission rates or patient length of stay.
Conclusion: This is the first systematic review with meta-analyses synthesizing the evidence of all ward round interventions targeted at improving patient and process outcomes. Results from this review should be used to inform guidelines for the 'ideal ward round'.
期刊介绍:
The British Journal of Surgery (BJS), incorporating the European Journal of Surgery, stands as Europe's leading peer-reviewed surgical journal. It serves as an invaluable platform for presenting high-quality clinical and laboratory-based research across a wide range of surgical topics. In addition to providing a comprehensive coverage of traditional surgical practices, BJS also showcases emerging areas in the field, such as minimally invasive therapy and interventional radiology.
While the journal appeals to general surgeons, it also holds relevance for specialty surgeons and professionals working in closely related fields. By presenting cutting-edge research and advancements, BJS aims to revolutionize the way surgical knowledge is shared and contribute to the ongoing progress of the surgical community.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


