Andrew Shepherd, Ata Jaffer, Angus Bruce, Daniel Chia, Prokar Dasgupta, Ben Challacombe
{"title":"Early clinical evaluation of the Hugo robotic-assisted surgery (RAS) for performing radical prostatectomy: an IDEAL stage 2 study.","authors":"Andrew Shepherd, Ata Jaffer, Angus Bruce, Daniel Chia, Prokar Dasgupta, Ben Challacombe","doi":"10.1136/bmjsit-2024-000360","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the feasibility and safety of the new Hugo robotic-assisted surgery (RAS) system for robotic-assisted radical prostatectomy (RARP), describing iterative changes in our operative technique-IDEAL stage 2.</p><p><strong>Design: </strong>Prospective, single-centre series.</p><p><strong>Setting: </strong>Tertiary urological unit in London, UK.</p><p><strong>Participants: </strong>Male patients diagnosed with clinically localised prostate cancer and suitable for RARP from February 2023 to May 2024.</p><p><strong>Main outcome measures: </strong>The primary outcome was to assess the safety of using the device without converting to the existing robotic platform (da Vinci), laparoscopy or open. Secondary outcomes assessed surgical (operative time, blood loss, time to catheter removal, complications), oncologic (surgical pathology and margin status) and early functional (continence) outcomes.</p><p><strong>Results: </strong>50 patients were included in the study. No cases required conversion to an existing robotic platform, laparoscopy or open, and there were no intraoperative surgical complications. Mean age was 60 years and mean prostate-specific antigen was 12.2 ng/mL. The mean operative time was 148 min and estimated blood loss was 168 mL. Mean length of stay was 1.5 days and mean length of catheter duration was 13 days. On final pathology, 18 patients (36%) had T3 disease and four had positive surgical margins (8%). The mean International Consultation on Incontinence Questionnaire-Urinary Incontinence score for urinary continence at 3 months was 7. There were six Clavien-Dindo grade 2 complications and two Clavien-Dindo 3a complications. There were four instances of recoverable, temporary device failure. Iterative improvements were made to docking setup, use of robotic instruments and reduction in robotic arm collisions.</p><p><strong>Conclusions: </strong>We demonstrated feasibility and the safe introduction of the Hugo RAS for RARP into an experienced robotic urological programme. Perioperative, early oncological and functional outcomes were similar to other early series. Further studies will aim to describe the learning curve with this robot and optimisation of surgical quality.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"7 1","pages":"e000360"},"PeriodicalIF":1.6000,"publicationDate":"2025-04-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11973793/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2024-000360","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To assess the feasibility and safety of the new Hugo robotic-assisted surgery (RAS) system for robotic-assisted radical prostatectomy (RARP), describing iterative changes in our operative technique-IDEAL stage 2.
Design: Prospective, single-centre series.
Setting: Tertiary urological unit in London, UK.
Participants: Male patients diagnosed with clinically localised prostate cancer and suitable for RARP from February 2023 to May 2024.
Main outcome measures: The primary outcome was to assess the safety of using the device without converting to the existing robotic platform (da Vinci), laparoscopy or open. Secondary outcomes assessed surgical (operative time, blood loss, time to catheter removal, complications), oncologic (surgical pathology and margin status) and early functional (continence) outcomes.
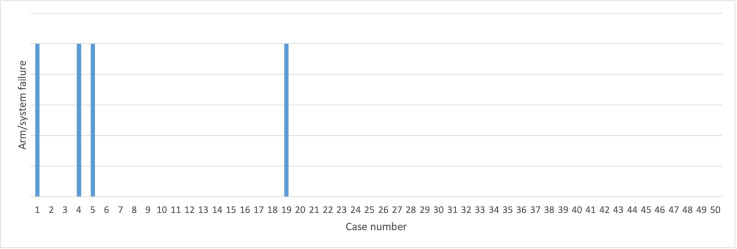
Results: 50 patients were included in the study. No cases required conversion to an existing robotic platform, laparoscopy or open, and there were no intraoperative surgical complications. Mean age was 60 years and mean prostate-specific antigen was 12.2 ng/mL. The mean operative time was 148 min and estimated blood loss was 168 mL. Mean length of stay was 1.5 days and mean length of catheter duration was 13 days. On final pathology, 18 patients (36%) had T3 disease and four had positive surgical margins (8%). The mean International Consultation on Incontinence Questionnaire-Urinary Incontinence score for urinary continence at 3 months was 7. There were six Clavien-Dindo grade 2 complications and two Clavien-Dindo 3a complications. There were four instances of recoverable, temporary device failure. Iterative improvements were made to docking setup, use of robotic instruments and reduction in robotic arm collisions.
Conclusions: We demonstrated feasibility and the safe introduction of the Hugo RAS for RARP into an experienced robotic urological programme. Perioperative, early oncological and functional outcomes were similar to other early series. Further studies will aim to describe the learning curve with this robot and optimisation of surgical quality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


