Irene Kang, Leah Naghi, Susan E Yost, Joanne Mortimer
{"title":"Clinical Actionability of Molecular Targets in Multi-Ethnic Breast Cancer Patients: A Retrospective Single-Institutional Study.","authors":"Irene Kang, Leah Naghi, Susan E Yost, Joanne Mortimer","doi":"10.1007/s40291-025-00777-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Precision oncology is making remarkable advancements in optimizing patient care by personalizing treatments. To date, the US Food and Drug Administration (FDA) has approved poly(ADP-ribose) polymerase inhibitors (PARPi) olaparib (Lynparza, AstraZeneca and Merck) and talazoparib (Talzenna, Pfizer Oncology Together™) for germline or somatic BRCA1/2-mutated metastatic breast cancer (BC) patients, and PI3K inhibitor alpelisib (Piqray, Novartis) plus fulvestrant for patients with hormone receptor-positive human epidermal growth factor receptor 2-negative (HR+HER2-) PIK3CA-mutated advanced BC. In addition, the FDA approved capivasertib (Trucap, AstraZeneca) for HR+HER2- locally advanced or metastatic BC patients with one or more AKT1, PIK3CA, or PTEN alterations. Finally, the FDA recently approved elacestrant (Orserdu, Stemline Therapeutics, Inc.) for postmenopausal patients with ER+ HER2- ESR1-mutated advanced or metastatic BC with disease progression following at least one line of endocrine therapy.</p><p><strong>Methods: </strong>This study presents a single institutional retrospective review of genomic reports of patients with BC. Analysis of genomic reports of 1361 BC sequencing reports was performed for 1010 patients with BC from 2013 to 2023 (23% of patients had multiple reports). Eligible patients had at least one primary or metastatic tumor. Multiple sequencing platforms were used for FFPE specimens including Tempus xT targeted next-generation sequencing (NGS), Foundation One Medicine, HopeSeq, Ashion Analytics GEM ExTra, and Exact Sciences Oncomap. Liquid biopsies were performed by Guardant, Tempus, and Foundation One Medicine. Chart reviews were performed to collect patient characteristics. BRCA1/2-mutated, metastatic BC patients who initiated treatment with olaparib or talazoparib, and PIK3CA-mutated, HR+ metastatic BC patients who initiated treatment with alpelisib were reported. In addition, patients with ESR1 or AKT1/PIK3CA/PTEN mutations were identified. Clinical outcomes, including progression-free survival (PFS) and overall survival (OS) were analyzed for BRCA1/2 and PIK3CA-mutated patients who received PARPi or alpelisib. Survival curves were generated using the Kaplan Meier method.</p><p><strong>Results: </strong>A cohort of 1010 BC patients with 1361 genomic reports was identified. A total of 935/1361 (69%) specimens were formalin-fixed paraffin-embedded (FFPE) tumor biopsies and 426/1361 (31%) were liquid biopsies. Receptor status included 65% HR+HER2-, 8% HR+HER2+, 4% HR-HER2+, and 23% TNBC. Racial and ethnic distribution of these patients included 50% non-Hispanic White, 26% Hispanic, 17% Asian, 6% African American, 1% other (Native Hawaiian or Other Pacific Islander, American Indian or Alaska Native, or unknown). Sequencing platforms included 30% Tempus xT, 31% Foundation One, 10% HopeSeq, 20% GEM ExTra, and 9% Exact Sciences. Liquid biopsies included 79% Guardant, 20% Tempus, and 1% Foundation One. Of 1010 patients, the most common mutations were TP53 (44%), PIK3CA (38%), ESR1 (14%), PTEN (12%), CCND1 (11%), FGFR1 (10%), CDH1 (10%), ERBB2 (9%), MYC (9%), FGF3 (8%), GATA3 (8%), FGF19 (8%), FGF4 (7%), ARID1A (6%), RB1 (5%), BRCA2 (5%), MAP3K1 (4%), AKT1 (4%), NF1 (4%), MLL3 (4%), ZNF703 (4%), CDKN2A (4%), BRCA1 (4%), MCL1 (3%), ATM (3%), PALB2 (1%), and CHEK2 (1%). The majority of reports with tumor mutation burden (TMB) results (97%) had low or intermediate TMB. A total of 784 actionable mutations in 1010 patients were reported, including 381/1010 (38%) PIK3CA; 144/1010 (14%) ESR1; 122/1010 (12%) PTEN; 48/1010 (5%) BRCA2; 36/1010 (4%) BRCA1; 41/1010 (4%) AKT1; and 12/1010 (1%) PALB2. Of the 96/1010 (10%) patients with BRCA1, BRCA2, or PALB2 mutations not including variants of uncertain significance (VUS), 33/96 (34.4%) received olaparib and 3/96 (3%) received talazoparib in the metastatic setting, and 28 were eligible for response (one had toxicity, two were lost to follow-up, and two went to hospice). Median PFS was 9.0 months and median OS was 21.8 months for patients receiving PARPi. Of the 381/1010 (38%) patients with PIK3CA mutations, 84/381 (22%) received alpelisib and 41 were eligible for response (22 had toxicity, 13 were discontinued, six were lost to follow-up, and two went to hospice). Median PFS was 7.9 months and median OS was 31.2 months for patients receiving alpelisib. A total of 544/1010 (54%) patients had AKT1, PIK3CA, or PTEN mutations which are now FDA approved for capivasertib in HR+HER2- metastatic BC patients. In addition, 144/1010 (14%) patients had ESR1 mutations which are FDA approved for elacestrant in HR+HER2- metastatic BC patients.</p><p><strong>Conclusions: </strong>In this study, a total of 784 clinically actionable mutations were reported for 1010 patients with genomic sequencing. Of these, 96/1010 (10%) patients had at least one actionable mutation in homologous recombination repair genes (BRCA1, BRCA2, PALB2) and 36/96 (37.5%) patients received PARP inhibitors (33 olaparib and three talazoparib). In addition, 381/1010 (38%) patients had at least one clinically actionable PIK3CA mutation, and 84/381 (22%) received alpelisib. Additionally, 544/1010 (54%) of patients had either AKT1 (41/1010), PIK3CA (381/1010), or PTEN (122/1010) alterations that were FDA approved in November 2023 for capivasertib in the treatment of HR+HER2- metastatic BC (MBC) patients. Furthermore, 144/1010 (14%) patients in this study had at least one ESR1 mutation, a clinically actionable mutation that was FDA approved in January 2023 for elacestrant in the treatment of ER+HER2- MBC patients (44% detected by liquid biopsy). Future studies are needed to determine the efficacy of elacestrant and capivasertib for patients with these mutations, and to tailor strategies for optimal patient quality of life and cancer outcome.</p>","PeriodicalId":49797,"journal":{"name":"Molecular Diagnosis & Therapy","volume":" ","pages":"393-405"},"PeriodicalIF":4.4000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12062054/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Molecular Diagnosis & Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40291-025-00777-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/7 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
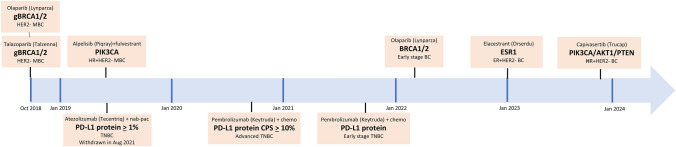
Background: Precision oncology is making remarkable advancements in optimizing patient care by personalizing treatments. To date, the US Food and Drug Administration (FDA) has approved poly(ADP-ribose) polymerase inhibitors (PARPi) olaparib (Lynparza, AstraZeneca and Merck) and talazoparib (Talzenna, Pfizer Oncology Together™) for germline or somatic BRCA1/2-mutated metastatic breast cancer (BC) patients, and PI3K inhibitor alpelisib (Piqray, Novartis) plus fulvestrant for patients with hormone receptor-positive human epidermal growth factor receptor 2-negative (HR+HER2-) PIK3CA-mutated advanced BC. In addition, the FDA approved capivasertib (Trucap, AstraZeneca) for HR+HER2- locally advanced or metastatic BC patients with one or more AKT1, PIK3CA, or PTEN alterations. Finally, the FDA recently approved elacestrant (Orserdu, Stemline Therapeutics, Inc.) for postmenopausal patients with ER+ HER2- ESR1-mutated advanced or metastatic BC with disease progression following at least one line of endocrine therapy.
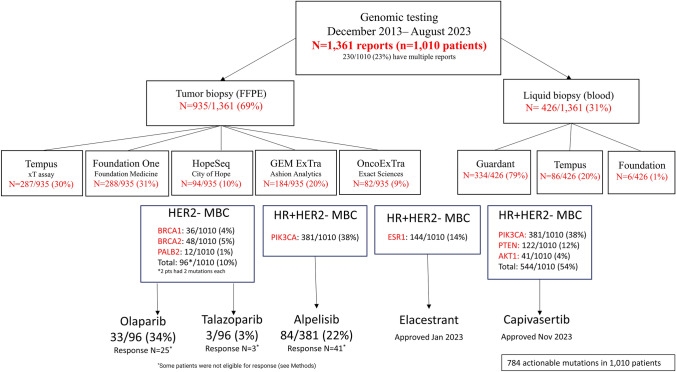
Methods: This study presents a single institutional retrospective review of genomic reports of patients with BC. Analysis of genomic reports of 1361 BC sequencing reports was performed for 1010 patients with BC from 2013 to 2023 (23% of patients had multiple reports). Eligible patients had at least one primary or metastatic tumor. Multiple sequencing platforms were used for FFPE specimens including Tempus xT targeted next-generation sequencing (NGS), Foundation One Medicine, HopeSeq, Ashion Analytics GEM ExTra, and Exact Sciences Oncomap. Liquid biopsies were performed by Guardant, Tempus, and Foundation One Medicine. Chart reviews were performed to collect patient characteristics. BRCA1/2-mutated, metastatic BC patients who initiated treatment with olaparib or talazoparib, and PIK3CA-mutated, HR+ metastatic BC patients who initiated treatment with alpelisib were reported. In addition, patients with ESR1 or AKT1/PIK3CA/PTEN mutations were identified. Clinical outcomes, including progression-free survival (PFS) and overall survival (OS) were analyzed for BRCA1/2 and PIK3CA-mutated patients who received PARPi or alpelisib. Survival curves were generated using the Kaplan Meier method.
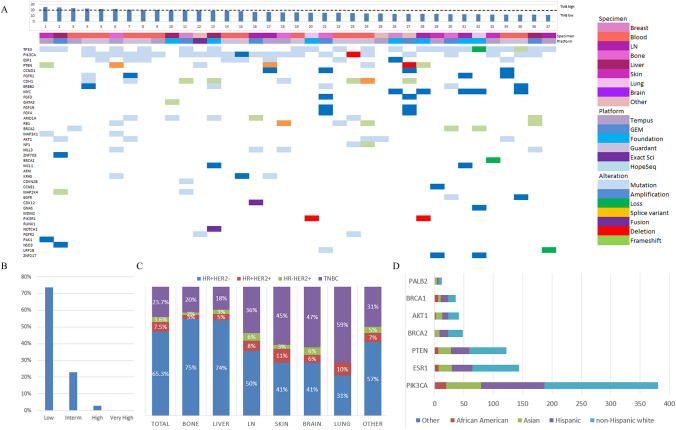
Results: A cohort of 1010 BC patients with 1361 genomic reports was identified. A total of 935/1361 (69%) specimens were formalin-fixed paraffin-embedded (FFPE) tumor biopsies and 426/1361 (31%) were liquid biopsies. Receptor status included 65% HR+HER2-, 8% HR+HER2+, 4% HR-HER2+, and 23% TNBC. Racial and ethnic distribution of these patients included 50% non-Hispanic White, 26% Hispanic, 17% Asian, 6% African American, 1% other (Native Hawaiian or Other Pacific Islander, American Indian or Alaska Native, or unknown). Sequencing platforms included 30% Tempus xT, 31% Foundation One, 10% HopeSeq, 20% GEM ExTra, and 9% Exact Sciences. Liquid biopsies included 79% Guardant, 20% Tempus, and 1% Foundation One. Of 1010 patients, the most common mutations were TP53 (44%), PIK3CA (38%), ESR1 (14%), PTEN (12%), CCND1 (11%), FGFR1 (10%), CDH1 (10%), ERBB2 (9%), MYC (9%), FGF3 (8%), GATA3 (8%), FGF19 (8%), FGF4 (7%), ARID1A (6%), RB1 (5%), BRCA2 (5%), MAP3K1 (4%), AKT1 (4%), NF1 (4%), MLL3 (4%), ZNF703 (4%), CDKN2A (4%), BRCA1 (4%), MCL1 (3%), ATM (3%), PALB2 (1%), and CHEK2 (1%). The majority of reports with tumor mutation burden (TMB) results (97%) had low or intermediate TMB. A total of 784 actionable mutations in 1010 patients were reported, including 381/1010 (38%) PIK3CA; 144/1010 (14%) ESR1; 122/1010 (12%) PTEN; 48/1010 (5%) BRCA2; 36/1010 (4%) BRCA1; 41/1010 (4%) AKT1; and 12/1010 (1%) PALB2. Of the 96/1010 (10%) patients with BRCA1, BRCA2, or PALB2 mutations not including variants of uncertain significance (VUS), 33/96 (34.4%) received olaparib and 3/96 (3%) received talazoparib in the metastatic setting, and 28 were eligible for response (one had toxicity, two were lost to follow-up, and two went to hospice). Median PFS was 9.0 months and median OS was 21.8 months for patients receiving PARPi. Of the 381/1010 (38%) patients with PIK3CA mutations, 84/381 (22%) received alpelisib and 41 were eligible for response (22 had toxicity, 13 were discontinued, six were lost to follow-up, and two went to hospice). Median PFS was 7.9 months and median OS was 31.2 months for patients receiving alpelisib. A total of 544/1010 (54%) patients had AKT1, PIK3CA, or PTEN mutations which are now FDA approved for capivasertib in HR+HER2- metastatic BC patients. In addition, 144/1010 (14%) patients had ESR1 mutations which are FDA approved for elacestrant in HR+HER2- metastatic BC patients.
Conclusions: In this study, a total of 784 clinically actionable mutations were reported for 1010 patients with genomic sequencing. Of these, 96/1010 (10%) patients had at least one actionable mutation in homologous recombination repair genes (BRCA1, BRCA2, PALB2) and 36/96 (37.5%) patients received PARP inhibitors (33 olaparib and three talazoparib). In addition, 381/1010 (38%) patients had at least one clinically actionable PIK3CA mutation, and 84/381 (22%) received alpelisib. Additionally, 544/1010 (54%) of patients had either AKT1 (41/1010), PIK3CA (381/1010), or PTEN (122/1010) alterations that were FDA approved in November 2023 for capivasertib in the treatment of HR+HER2- metastatic BC (MBC) patients. Furthermore, 144/1010 (14%) patients in this study had at least one ESR1 mutation, a clinically actionable mutation that was FDA approved in January 2023 for elacestrant in the treatment of ER+HER2- MBC patients (44% detected by liquid biopsy). Future studies are needed to determine the efficacy of elacestrant and capivasertib for patients with these mutations, and to tailor strategies for optimal patient quality of life and cancer outcome.
期刊介绍:
Molecular Diagnosis & Therapy welcomes current opinion articles on emerging or contentious issues, comprehensive narrative reviews, systematic reviews (as outlined by the PRISMA statement), original research articles (including short communications) and letters to the editor. All manuscripts are subject to peer review by international experts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


