Risk stratification during antenatal care failed to identify most mothers who experienced adverse pregnancy outcomes: A prospective study from Kakamega County, Kenya.
IF 2.3 4区 医学Q2 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
Jan E Cooper, Margaret Kruk, David Kapaon, Kennedy Opondo, Jacinta Nzinga, Rose J Kosgei, Kevin Croke
{"title":"Risk stratification during antenatal care failed to identify most mothers who experienced adverse pregnancy outcomes: A prospective study from Kakamega County, Kenya.","authors":"Jan E Cooper, Margaret Kruk, David Kapaon, Kennedy Opondo, Jacinta Nzinga, Rose J Kosgei, Kevin Croke","doi":"10.1111/tmi.14110","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Risk stratification of pregnancies informs clinical care globally. Yet recent research has cast doubt on the ability of currently used population-level risk measures to accurately predict poor outcomes at the individual level. We examine the assumption that existing forms of risk stratification can successfully identify women likely to develop complications during delivery in a rural setting in Kenya.</p><p><strong>Methods: </strong>We conducted a prospective observational study of 19,653 pregnant women in Kakamega County in Western Kenya. Women were contacted three times during the perinatal period and surveyed about provider-identified risks and self-assessed concerns about pregnancy complications, delivery process outcomes, and adverse delivery outcomes. Measures of risk were derived from women's self-reporting. We compared delivery process outcomes and adverse delivery outcomes between high- and low-risk pregnancies, and between women with and without expressed concerns about delivery complications. Delivery process outcomes included intrapartum referral, unplanned caesarean section, blood transfusion, hysterectomy, or admission to an intensive care unit. Adverse delivery outcomes included stillbirth, neonatal mortality, and maternal mortality. We reported means and confidence intervals for each category, and tested for differences using bivariate linear regression.</p><p><strong>Results: </strong>Thirty-eight percent of pregnancies had at least one risk factor consistent with a high risk pregnancy; the remaining 62% were low risk by this criteria. Rates of most adverse process outcomes and delivery outcomes were higher among pregnancies with known risks. However, 64.5% of maternal deaths and 54.8% of all deaths in the sample took place among pregnancies characterised as low risk.</p><p><strong>Conclusions: </strong>Risk stratification using existing indicators of risk during pregnancy is inadequate to identify women at risk of adverse health outcomes in this setting.</p>","PeriodicalId":23962,"journal":{"name":"Tropical Medicine & International Health","volume":" ","pages":"531-538"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136940/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tropical Medicine & International Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tmi.14110","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Risk stratification of pregnancies informs clinical care globally. Yet recent research has cast doubt on the ability of currently used population-level risk measures to accurately predict poor outcomes at the individual level. We examine the assumption that existing forms of risk stratification can successfully identify women likely to develop complications during delivery in a rural setting in Kenya.
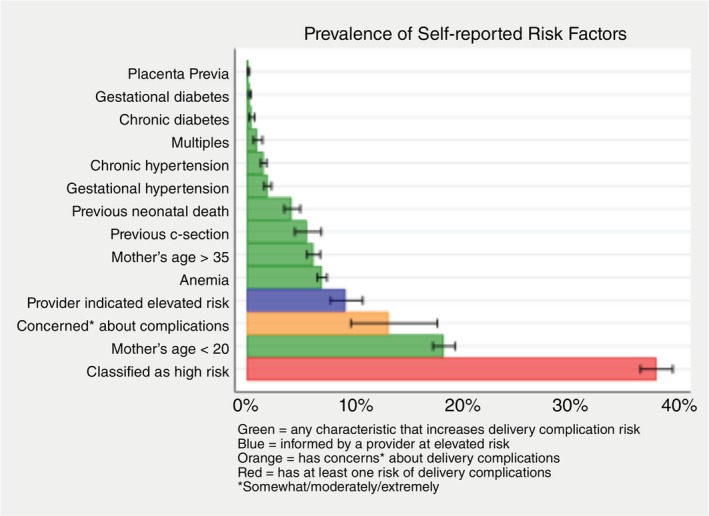
Methods: We conducted a prospective observational study of 19,653 pregnant women in Kakamega County in Western Kenya. Women were contacted three times during the perinatal period and surveyed about provider-identified risks and self-assessed concerns about pregnancy complications, delivery process outcomes, and adverse delivery outcomes. Measures of risk were derived from women's self-reporting. We compared delivery process outcomes and adverse delivery outcomes between high- and low-risk pregnancies, and between women with and without expressed concerns about delivery complications. Delivery process outcomes included intrapartum referral, unplanned caesarean section, blood transfusion, hysterectomy, or admission to an intensive care unit. Adverse delivery outcomes included stillbirth, neonatal mortality, and maternal mortality. We reported means and confidence intervals for each category, and tested for differences using bivariate linear regression.
Results: Thirty-eight percent of pregnancies had at least one risk factor consistent with a high risk pregnancy; the remaining 62% were low risk by this criteria. Rates of most adverse process outcomes and delivery outcomes were higher among pregnancies with known risks. However, 64.5% of maternal deaths and 54.8% of all deaths in the sample took place among pregnancies characterised as low risk.
Conclusions: Risk stratification using existing indicators of risk during pregnancy is inadequate to identify women at risk of adverse health outcomes in this setting.
期刊介绍:
Tropical Medicine & International Health is published on behalf of the London School of Hygiene and Tropical Medicine, Swiss Tropical and Public Health Institute, Foundation Tropical Medicine and International Health, Belgian Institute of Tropical Medicine and Bernhard-Nocht-Institute for Tropical Medicine. Tropical Medicine & International Health is the official journal of the Federation of European Societies for Tropical Medicine and International Health (FESTMIH).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


