Eyal Talor, József Tímár, Philip Lavin, John Cipriano, Dusan Markovic, Andrea Ladányi, Andrey Karpenko, Igor Bondarenko, Srboljub Stosic, Hrvoje Sobat, Aliaksandr Zhukavets, Nazim Imamovic, Chih-Yen Chien, Magdalena Bankowska-Wozniak, Mihály Kisely, Rajko Jovic, James Edward Massey Young, Sheng-Po Hao
{"title":"Neoadjuvant leukocyte interleukin injection immunotherapy improves overall survival in low-risk locally advanced head and neck squamous cell carcinoma -the <i>IT-MATTERS</i> study.","authors":"Eyal Talor, József Tímár, Philip Lavin, John Cipriano, Dusan Markovic, Andrea Ladányi, Andrey Karpenko, Igor Bondarenko, Srboljub Stosic, Hrvoje Sobat, Aliaksandr Zhukavets, Nazim Imamovic, Chih-Yen Chien, Magdalena Bankowska-Wozniak, Mihály Kisely, Rajko Jovic, James Edward Massey Young, Sheng-Po Hao","doi":"10.3389/pore.2025.1612084","DOIUrl":null,"url":null,"abstract":"<p><p>The randomized controlled pivotal phase 3 study evaluated efficacy and safety of neoadjuvant complex biologic, Leukocyte Interleukin Injection (LI), administered for 3 consecutive weeks pre-surgery, in treatment naïve resectable locally advanced primary squamous cell carcinoma of oral cavity and soft palate. Randomization 3:1:3 to LI+/-CIZ (cyclophosphamide, indomethacin, and zinc)+SOC, or SOC (standard of care) alone. LI-treated patients received 400 IU (as interleukin-2 equivalent; 200 IU peritumorally, 200 IU perilymphatically) sequentially, daily 5 days/week for 3 weeks before surgery. All subjects were to receive SOC. Post-surgery, patients with low risk for recurrence were to receive radiotherapy, while those with high risk received concurrent chemoradiotherapy. Median follow-up was 56 months. There were 923 ITT (Intent-to-Treat) subjects (380 ITT low-risk and 467 ITT high-risk). Pre-surgery objective early response (45 objective early responders; 5 complete responses [CRs], 40 partial responses [PRs], confirmed by pathology at surgery. LI (+/- CIZ) had 8.5% objective early responders (45/529 ITT) and 16% objective early responders (34/212 ITT low-risk) vs. no reported SOC objective early responders (0/394 ITT). Objective early responders significantly lowered death rate to 22.2% (ITT LI-treated), 12.5% (ITT low-risk LI + CIZ + SOC), while the ITT low-risk SOC death rate was 48.7%. Thus, objective early response impacted overall survival (OS); proportional hazard ratios were 0.348 (95% CI: 0.152-0.801) for ITT low-risk LI-treated, 0.246 (95% CI: 0.077-0.787) for ITT low-risk LI + CIZ + SOC. ITT low-risk LI + CIZ + SOC demonstrated significant OS advantage vs. ITT low-risk SOC (unstratified log-rank p = 0.048; Cox hazard ratio = 0.68; 95% CI: 0.48-0.95, Wald p = 0.024 [controlling for tumor stage, tumor location, and geographic region]). Absolute OS advantage increased over time for ITT low-risk (LI + CIZ + SOC)-treated vs. ITT low-risk SOC: reaching 14.1% (62.7% vs. 48.6%) at 60 months, with 46.5 months median OS advantage (101.7 months vs. 55.2 months), respectively. Quality of life benefit for complete responders sustained for >3 years post LI treatment. Percent treatment-emergent adverse events were comparable among all treated groups. No excess safety issues were reported for LI over SOC alone post-surgery. NCT01265849, EUDRA:2010-019952-35.</p>","PeriodicalId":19981,"journal":{"name":"Pathology & Oncology Research","volume":"31 ","pages":"1612084"},"PeriodicalIF":2.3000,"publicationDate":"2025-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968324/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pathology & Oncology Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/pore.2025.1612084","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
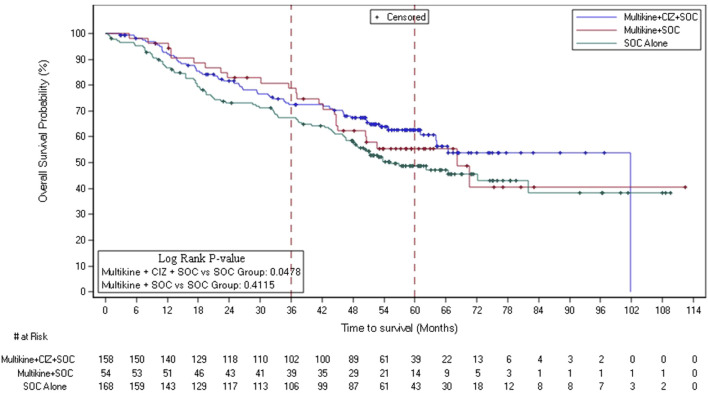
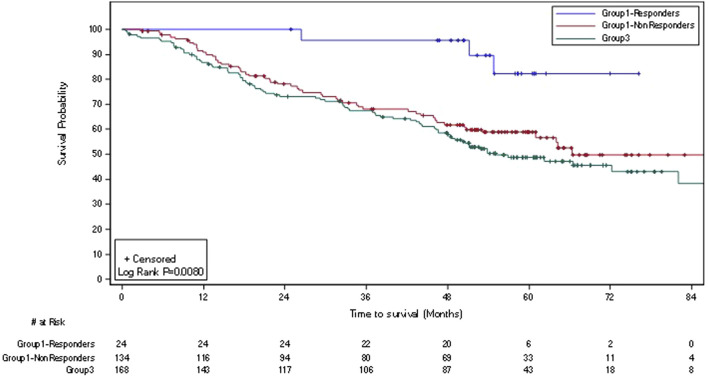
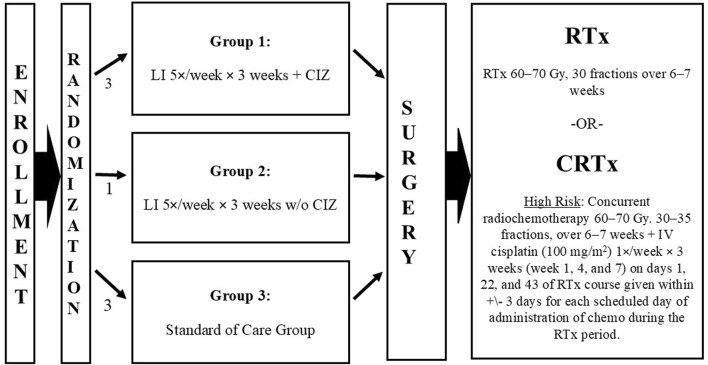
The randomized controlled pivotal phase 3 study evaluated efficacy and safety of neoadjuvant complex biologic, Leukocyte Interleukin Injection (LI), administered for 3 consecutive weeks pre-surgery, in treatment naïve resectable locally advanced primary squamous cell carcinoma of oral cavity and soft palate. Randomization 3:1:3 to LI+/-CIZ (cyclophosphamide, indomethacin, and zinc)+SOC, or SOC (standard of care) alone. LI-treated patients received 400 IU (as interleukin-2 equivalent; 200 IU peritumorally, 200 IU perilymphatically) sequentially, daily 5 days/week for 3 weeks before surgery. All subjects were to receive SOC. Post-surgery, patients with low risk for recurrence were to receive radiotherapy, while those with high risk received concurrent chemoradiotherapy. Median follow-up was 56 months. There were 923 ITT (Intent-to-Treat) subjects (380 ITT low-risk and 467 ITT high-risk). Pre-surgery objective early response (45 objective early responders; 5 complete responses [CRs], 40 partial responses [PRs], confirmed by pathology at surgery. LI (+/- CIZ) had 8.5% objective early responders (45/529 ITT) and 16% objective early responders (34/212 ITT low-risk) vs. no reported SOC objective early responders (0/394 ITT). Objective early responders significantly lowered death rate to 22.2% (ITT LI-treated), 12.5% (ITT low-risk LI + CIZ + SOC), while the ITT low-risk SOC death rate was 48.7%. Thus, objective early response impacted overall survival (OS); proportional hazard ratios were 0.348 (95% CI: 0.152-0.801) for ITT low-risk LI-treated, 0.246 (95% CI: 0.077-0.787) for ITT low-risk LI + CIZ + SOC. ITT low-risk LI + CIZ + SOC demonstrated significant OS advantage vs. ITT low-risk SOC (unstratified log-rank p = 0.048; Cox hazard ratio = 0.68; 95% CI: 0.48-0.95, Wald p = 0.024 [controlling for tumor stage, tumor location, and geographic region]). Absolute OS advantage increased over time for ITT low-risk (LI + CIZ + SOC)-treated vs. ITT low-risk SOC: reaching 14.1% (62.7% vs. 48.6%) at 60 months, with 46.5 months median OS advantage (101.7 months vs. 55.2 months), respectively. Quality of life benefit for complete responders sustained for >3 years post LI treatment. Percent treatment-emergent adverse events were comparable among all treated groups. No excess safety issues were reported for LI over SOC alone post-surgery. NCT01265849, EUDRA:2010-019952-35.
期刊介绍:
Pathology & Oncology Research (POR) is an interdisciplinary Journal at the interface of pathology and oncology including the preclinical and translational research, diagnostics and therapy. Furthermore, POR is an international forum for the rapid communication of reviews, original research, critical and topical reports with excellence and novelty. Published quarterly, POR is dedicated to keeping scientists informed of developments on the selected biomedical fields bridging the gap between basic research and clinical medicine. It is a special aim for POR to promote pathological and oncological publishing activity of colleagues in the Central and East European region. The journal will be of interest to pathologists, and a broad range of experimental and clinical oncologists, and related experts. POR is supported by an acknowledged international advisory board and the Arányi Fundation for modern pathology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


