Detection of fluid responsiveness by changes of perfusion index and pleth-variability index during passive leg raising in spontaneously breathing post-surgical patients: a prospective interventional study.
Simon Rauch, Paolo Mario Seraglio, Tomas Dal Cappello, Giulia Roveri, Markus Falk, Matthias Bock
{"title":"Detection of fluid responsiveness by changes of perfusion index and pleth-variability index during passive leg raising in spontaneously breathing post-surgical patients: a prospective interventional study.","authors":"Simon Rauch, Paolo Mario Seraglio, Tomas Dal Cappello, Giulia Roveri, Markus Falk, Matthias Bock","doi":"10.1007/s10877-025-01292-0","DOIUrl":null,"url":null,"abstract":"<p><p>Predicting fluid responsiveness is crucial in treating circulatory failure, as only about half of patients benefit from volume expansion by increasing cardiac output (CO). Dynamic tests like passive leg raising (PLR) are preferred over static parameters. While PLR reliably predicts fluid responsiveness, it typically requires invasive measurement of stroke volume (SV) or CO. The perfusion index (PI) and pleth variability index (PVI) are non-invasive metrics derived from oxygen saturation signals. PI has been shown to correlate with SV, and PVI has predicted fluid responsiveness in mechanically ventilated patients, but their role in spontaneously breathing patients remains unclear. This study aimed to assess whether PI and PVI could predict fluid responsiveness in post-surgical, spontaneously breathing patients during a PLR test. The hypothesis was that PI would increase and PVI would decrease in fluid responders. The prospective study included spontaneously breathing patients after major abdominal surgery in the ICU of Merano Hospital, Italy. SV and CO were measured using the FloTrac™ system, and PI and PVI were assessed using the Radical 7<sup>®</sup> monitor. Patients were considered responders if SV increased by ≥ 10% during the PLR test. Of the 47 patients enrolled, 23 (48.9%) were fluid responders. The percentage change in PI from baseline to 60 s into the PLR test was + 41.2% in responders and + 11.3% in non-responders. A PI increase of ≥ 23% predicted responders with 70% sensitivity and 75% specificity, with an area under the ROC curve of 0.74. Twenty-two patients (47%) were inside the grey zone. PVI did not differ significantly between groups. In conclusion, PI could be a helpful non-invasive tool for predicting fluid responsiveness during a PLR test in spontaneously breathing patients, though its diagnostic accuracy appears to be moderate.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"929-936"},"PeriodicalIF":2.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474676/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-025-01292-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
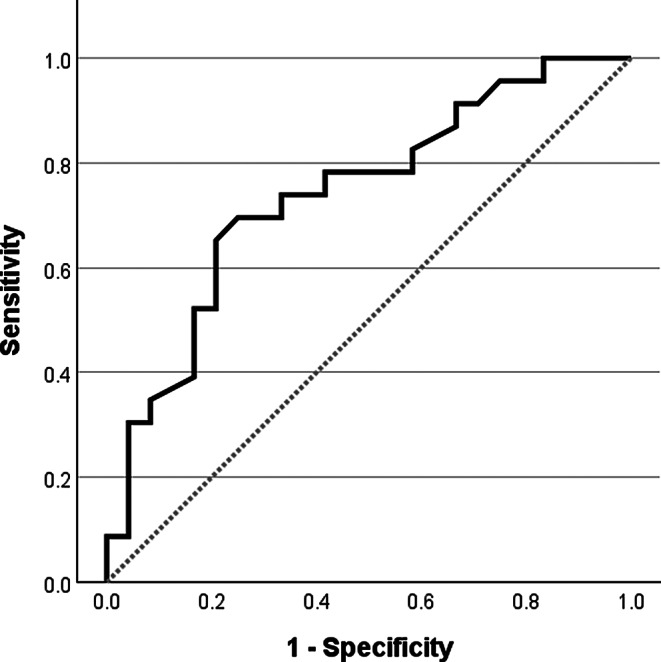
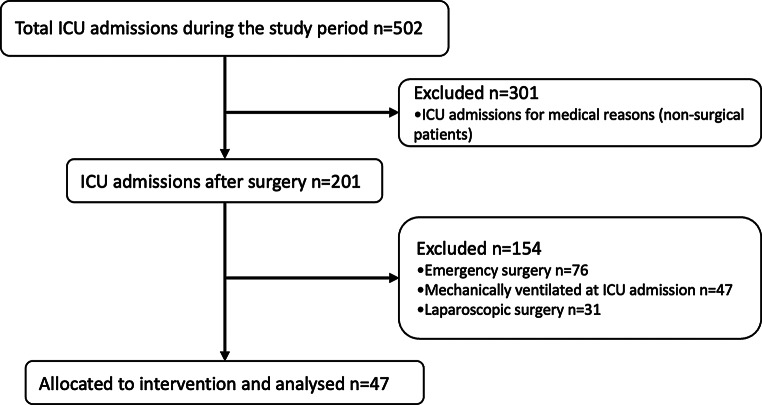
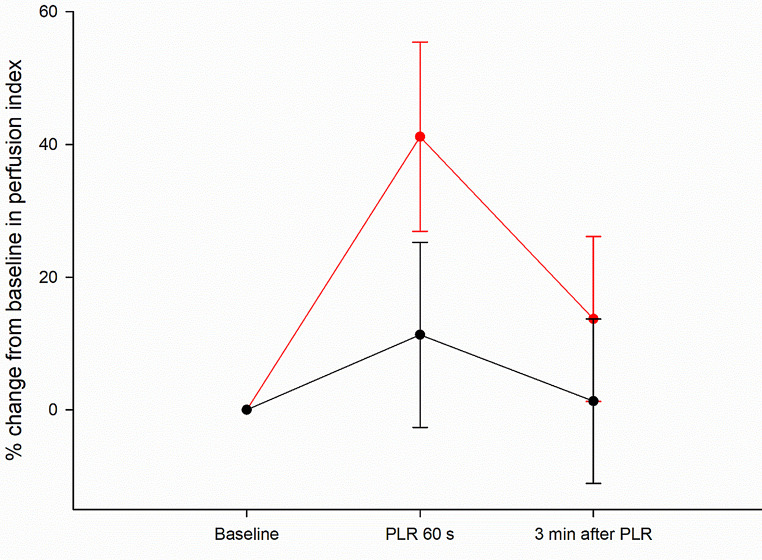
Predicting fluid responsiveness is crucial in treating circulatory failure, as only about half of patients benefit from volume expansion by increasing cardiac output (CO). Dynamic tests like passive leg raising (PLR) are preferred over static parameters. While PLR reliably predicts fluid responsiveness, it typically requires invasive measurement of stroke volume (SV) or CO. The perfusion index (PI) and pleth variability index (PVI) are non-invasive metrics derived from oxygen saturation signals. PI has been shown to correlate with SV, and PVI has predicted fluid responsiveness in mechanically ventilated patients, but their role in spontaneously breathing patients remains unclear. This study aimed to assess whether PI and PVI could predict fluid responsiveness in post-surgical, spontaneously breathing patients during a PLR test. The hypothesis was that PI would increase and PVI would decrease in fluid responders. The prospective study included spontaneously breathing patients after major abdominal surgery in the ICU of Merano Hospital, Italy. SV and CO were measured using the FloTrac™ system, and PI and PVI were assessed using the Radical 7® monitor. Patients were considered responders if SV increased by ≥ 10% during the PLR test. Of the 47 patients enrolled, 23 (48.9%) were fluid responders. The percentage change in PI from baseline to 60 s into the PLR test was + 41.2% in responders and + 11.3% in non-responders. A PI increase of ≥ 23% predicted responders with 70% sensitivity and 75% specificity, with an area under the ROC curve of 0.74. Twenty-two patients (47%) were inside the grey zone. PVI did not differ significantly between groups. In conclusion, PI could be a helpful non-invasive tool for predicting fluid responsiveness during a PLR test in spontaneously breathing patients, though its diagnostic accuracy appears to be moderate.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


